Concern for septic arthritis
Duration:
CC: erythema limited ROM and pain
O/C/P: ((s/g-c/i-w/i/u))
PP: Swelling/fullness around the joint, Malaise, fatigue
PN: DENIES Fever ± chills
mHx: gout / pseudogout, Recent infection, Immunosuppression: diabetes, steroids, chemo, HIV, rthritis / chronic joint disease, Skin wounds / cellulitis, Prosthetic joint
sHx: IVDU
initial DATA: CBC,CMP,ESR/CRP, Bcx x2 and lactate if febrile, X-ray
past Micro:
MEDS: Immunosuppressants,antibiotics
COURSE:
DDX: cellulitis, Diabetic foot infections_ (vascular insufficiency)
Plan
consult Ortho for arthrocentesis +/- wash out, fluid studies (WBC >50k)
ID consult for Abx management
Hold AC if pt taking
hold antibiotics before arthrocentesis unless unstable
IV Abx only if unstable ( septic shock ) CFPM+VANC
Trend CBC,BMP daily
follow up blood cultures
PT/OT when possible
trend fever curve
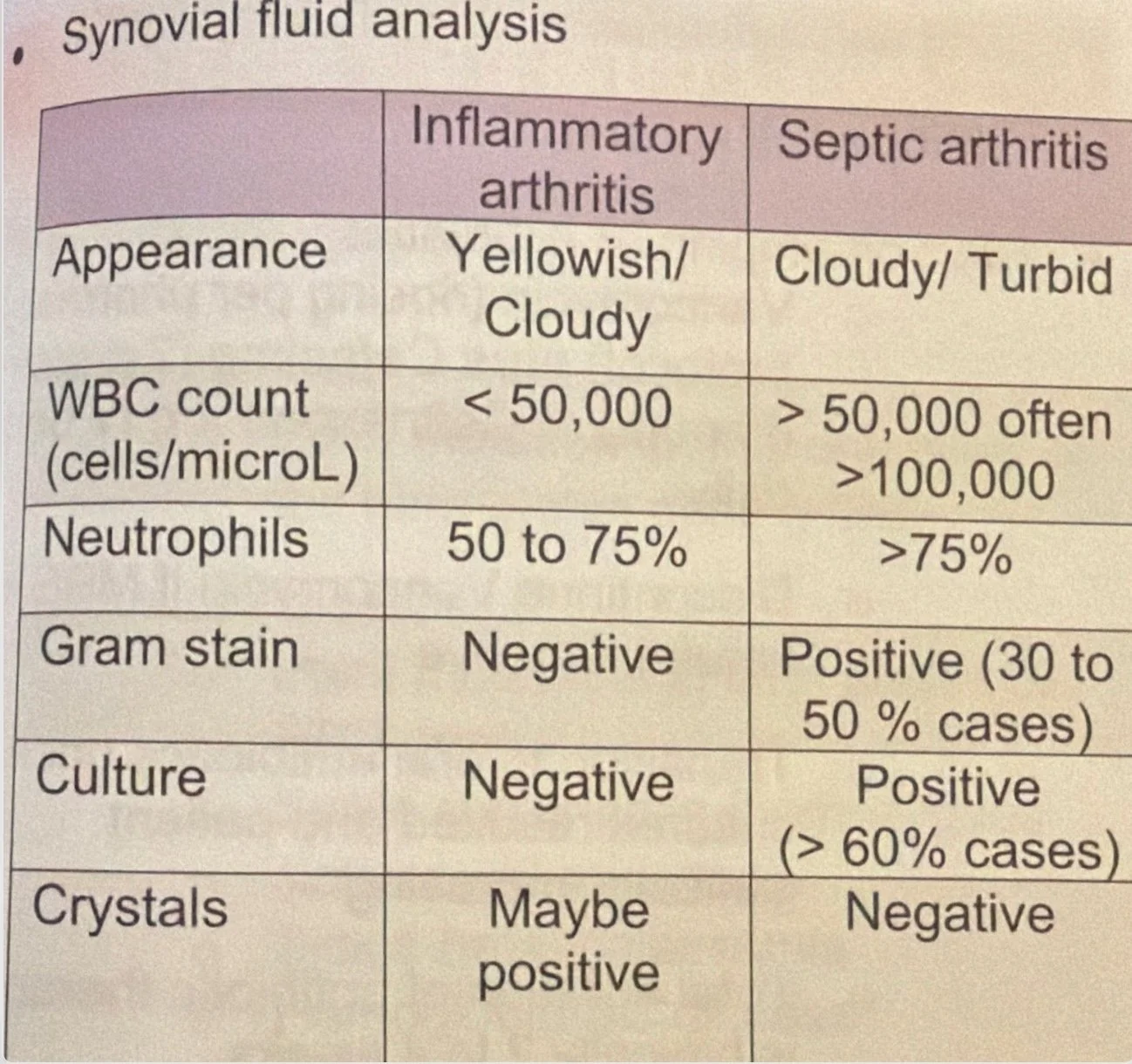
** f/u Synovial Fluid WBC count, Neutrophils, stain and culture
Note
if not getting better might need MRI for complication
abx duration: usually 3-4 weeks
Synovial fluid WBC count >50,000/μL with >90% neutrophils is the classic finding, also Absence of crystals — Negative birefringent crystals (gout) or positively birefringent crystals (pseudogout)
Cellulitis
-- __Days
-- cc: Unilateral erythema
-- sudden/gradual onset, constant/intermittent course, worsening/improving /unchanged Progression
-- PP:
-- PN: fever, chills, w/o improves on elevation, rapid spread, Severe pain out of proportion, Deep muscle pain, no ulcers ,
-- PE: UL erythema (no pain out of proportion, crepitus, ulcers)
-- Data: CBC, BMP, LFTs, BCx if systemic, US (DVT)
-- Hx: previous Micro, cellulite, imunocopmpremised , IVDU, DM
-- Meds:
-- DDX: erysipelas, pyomyositis, necrotizing fasciitis, osteomyelitis, venous stasis
-- Hospital course:
Plan:
mild: PO Cephalexin/Keflex 500 mg QID (( Localized infection and No systemic signs ))
mild + purulence: (Bactrim) 1–2 DS BID (cover MRSA)
Mod/Severe: IV Cefazolin/Ancef 2g q8h (SIRS criteria ≤2)
Mod/Severe + purulence : IV Cefazolin 2g q8h + Vanc
Duration 5 days if improvement, if not Extend to 10–14 days
if abscess present → Incision & Drainage is essential + Vanco sould be on regiment
F/U cultures
trend CBC,RFP daily
would care consult at place
PT/OT to eval and treat
if become septic broaden tx: vancomycin plus meropenum
CT if c/f nec fasc, pyomyositis, or osteomyelitis
if necrotizing fasciitis urgent surgery consultation (rapid spread of infection, crepitus, air in tissues on imaging, or pain out of proportion to exam) will need CT w/contrast
Plan/Note
Blood cultures ONLY if systemic signs of infection or immunodeficiency
Mild, not meeting SIRS, Immunocompetent, no systemic signs , low suspicion for MRSA -> Cephalexin or Dicloxacillin both 500 mg QID (PO), if Purulent / MRSA suspected -> TMP-SMX (Bactrim) 1–2 DS BID or Doxycycline 100 mg BID
Moderate/severe ≥2 SIRS (systemic signs of infection)-> Cefazolin 2g q8h, and if purulent/MRSA suspected add Vanco, PO step down: cephalexin 500 mg q6h or 1000mg q8h and for MRSA Linezolid 600 mg PO BID
Severe cellulitis / purulent (penetrating trauma, MRSA risk factors, injection drug use, purulent drainage, or SIRS): add Vancomycin and then step down: TMP/SMX 1-2 DS tabs BID or Doxycycline 100 mg BID or Linezolid 600 mg BID
Duration is 5 days if clinical improvement occurs; extend if not improving to Extend to 10–14 days
If abscess present → Incision & Drainage (I&D) is essential + Vanco sould be on regiment
if become septic broaden tx: vancomycin plus meropenum
CT/MRI w/contrast: if necrotizing fasciitis, pyomyositis or osteomyelitis suspected
if necrotizing fasciitis urgent surgery consultation (rapid spread of infection, crepitus, air in tissues on imaging, or pain out of proportion to exam) will need CT w/contrast
mild has Localized skin infection and No systemic signs of infection , tx po
Moderate WITH systemic signs of infection - Fever >38°C, Tachycardia >90, Tachypnea >20, Leukocytosis. tx iv
for mild other abx options are Dicloxacillin 500 mg QID or Amoxicillin-clavulanate 875 mg BID for 5 days
Pathogens: Streptococcus species: Group A (most common), B, C, G, Staphylococcus aureus (including MSSA and MRSA)
Non-purulent Think Streptococcus
Purulence (abscess or boil)? Think Staphylococcus
Typically improvement is not seen until >48 hours of antibiotics, usually longer
Bilateral lower extremity cellulitis is RARE usually unilateral
Unlikely cellulitis as erythema fades after pt raises the leg for 1–2 minutes.