Small Bowel Obstruction (SBO)
Mechanical obstruction of the small intestine — most commonly from post-surgical adhesions
Symptoms / Associated Sx
Colicky, crampy periumbilical or diffuse abdominal pain (intermittent waves)
Nausea, vomiting (bilious early; feculent in late/complete obstruction)
Abdominal distension; obstipation (complete obstruction)
High-pitched or tinkling bowel sounds early; absent bowel sounds late (strangulation)
Denies
Prior abdominal surgery (raises malignancy or hernia concern as etiology)
Peritoneal signs (rules out strangulation/perforation if truly absent — do not be reassured)
Passage of flatus or stool (rules out complete obstruction)
Social History (SHx)
Prior abdominal surgeries (adhesions), hernia repair, IBD or malignancy history, prior SBO, radiation to abdomen/pelvis.
Main Etiology
Adhesions (~60–75%) — prior surgical or inflammatory
Hernias (incarcerated/strangulated) — most common without prior surgery
Malignancy (primary SB, peritoneal carcinomatosis, metastatic)
Crohn's disease (stricture, inflammatory mass)
Intussusception (adult — often pathologic lead point); gallstone ileus; volvulus
Most Common DDx
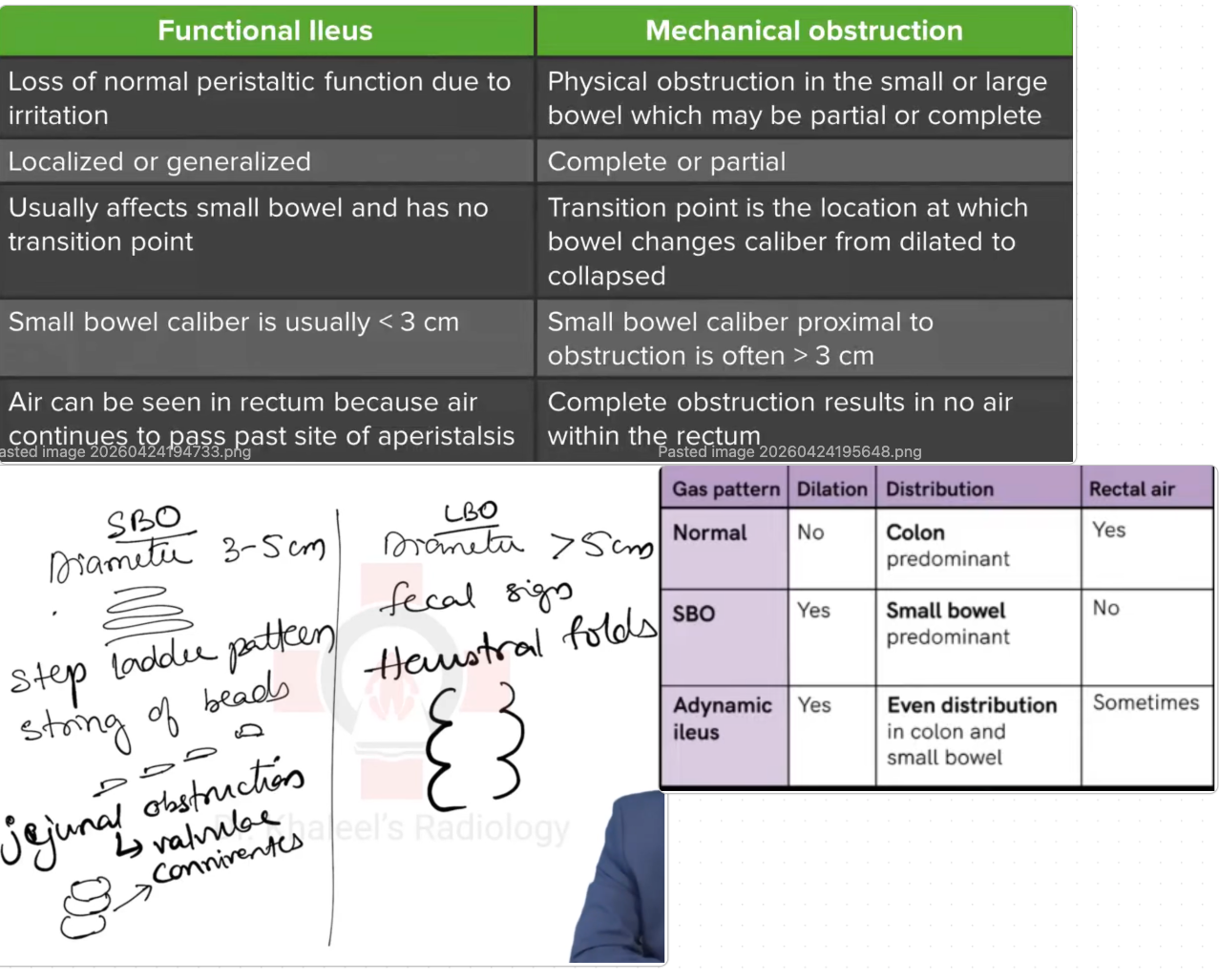
Ileus / paralytic ileus (no mechanical obstruction; gas throughout small AND large bowel on AXR; no transition point on CT; history of surgery, narcotics, metabolic derangement)
Large bowel obstruction (colonic dilation predominant; no or minimal small bowel dilation; colon gas distal to obstruction usually absent; CT transition point in colon)
Acute mesenteric ischemia (severe abdominal pain out of proportion to exam; older patient with vascular risk factors; lactate elevated; CT angiography shows mesenteric vessel occlusion)
Ogilvie's syndrome / colonic pseudo-obstruction (massively dilated colon without mechanical obstruction; immobility + narcotics + metabolic precipitants; no transition point on CT)
Intussusception (adult — must rule out lead point malignancy; CT shows target sign; bowel within bowel)
Volvulus (sigmoid or cecal; coffee bean sign on AXR; bird's beak on CT; decompression + elective surgery)
DATA
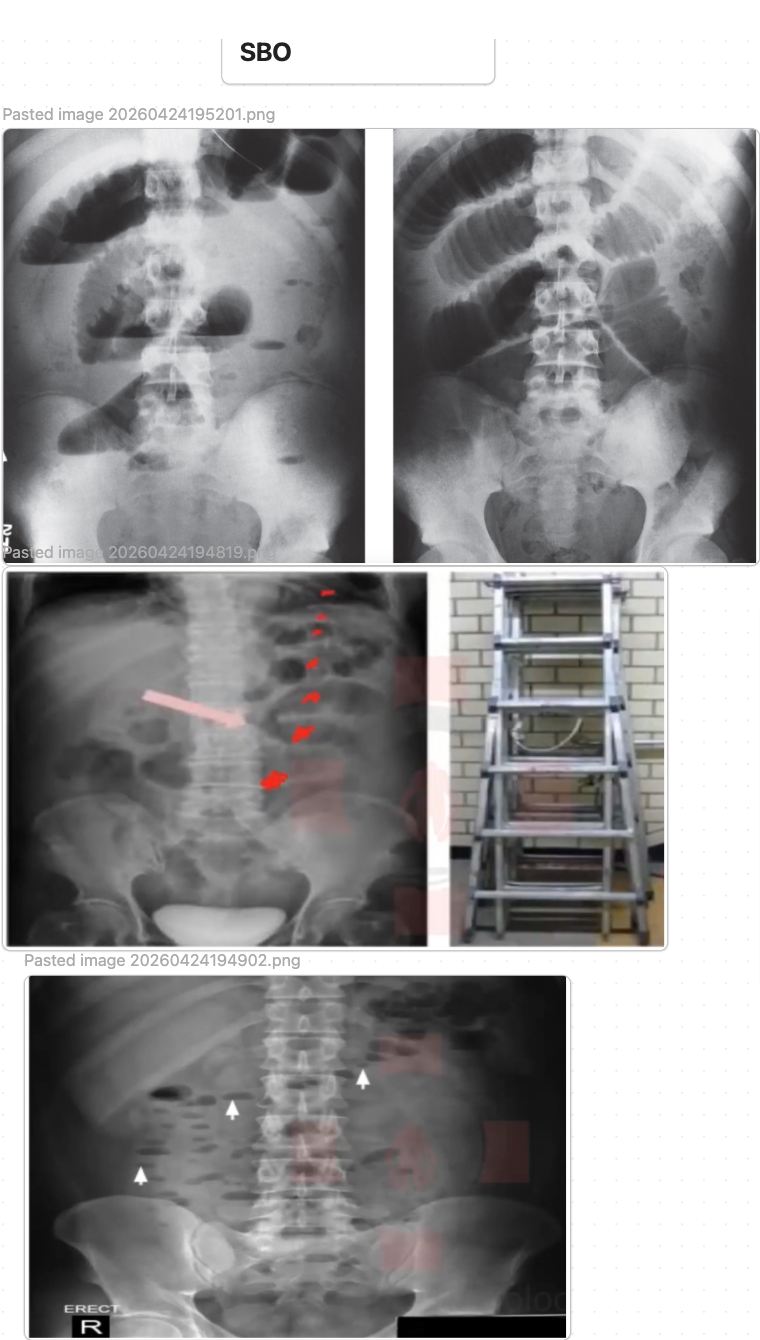
CBC, BMP, lactate; plain AXR (dilated SB loops, air-fluid levels, step-ladder pattern; no colonic gas in complete SBO)
CT abdomen/pelvis with IV contrast (gold standard — level, cause, strangulation signs: pneumatosis, portal venous gas, mesenteric edema)
Water-soluble contrast study (gastrografin) — diagnostic and therapeutic
Home Meds
Opioids (constipation — hold; reassess); anticholinergics (hold); anticoagulants (hold if surgery anticipated)
Plan
NPO; NGT decompression (low-intermittent suction); IV fluid resuscitation (NS or LR); Foley for UO monitoring; surgery consult immediately
Non-operative management (partial/adhesive SBO, no strangulation):
NGT + NPO + IVF × 24–48h trial
Gastrografin 100–150 mL via NGT — therapeutic (~30–40% resolution) + diagnostic; contrast to colon within 24h = 97% spontaneous resolution
Urgent/emergent surgery: Strangulation signs; complete SBO not resolving; incarcerated/strangulated hernia; closed-loop obstruction
Electrolyte replacement (K+, Mg2+, phos); serial abdominal exams q4–8h; daily CBC, BMP, lactate
Trend fever curve; rising WBC/lactate → escalate surgery urgency; PT/OT post-operatively
Discharge: Clear liquids → low-fiber; avoid large bolus meals; activity restrictions per surgery; return precautions: worsening pain, vomiting, inability to pass gas; surgery follow-up 2 weeks
Red Flags
Strangulation: fever + WBC elevation + peritoneal signs + lactate rise → emergent surgery
Pneumatosis intestinalis or portal venous gas on CT → ischemic bowel → emergent surgery
Closed-loop obstruction on CT → very high strangulation risk → urgent surgery
Incarcerated hernia → emergent surgery; strangulated hernia → true emergency
Complete SBO not improving after 48h → operative intervention
Senior IM Resident Pearls
Early strangulation can be clinically silent — normal WBC and mild pain do not exclude ischemia; CT essential for any SBO with tachycardia or elevated lactate
Gastrografin challenge: 100–150 mL via NGT; contrast to colon within 24h = 97% spontaneous resolution; also therapeutic (osmotic edema reduction)
Gallstone ileus: Rigler's triad — pneumobilia + SBO + ectopic calcification; elderly women; requires surgical enterotomy
Common mistake: Delaying surgery for one more day of conservative management when lactate is rising or fever present
Common mistake: NGT without suction — decompression requires active low-intermittent suction
Large Bowel Obstruction (LBO)
Mechanical obstruction of the colon — most commonly from malignancy or sigmoid volvulus
Symptoms / Associated Sx
Progressive severe abdominal distension; obstipation; crampy lower abdominal pain
Nausea and vomiting (late — feculent in distal obstruction)
Tympanic abdomen on percussion
Denies
Peritoneal signs (rules out perforation if absent)
Passage of flatus or stool (confirms obstruction)
Social History (SHx)
Age >50 + change in bowel habits + weight loss (colon cancer), prior colon cancer or IBD, chronic constipation, institutionalized/elderly + high-fiber diet (sigmoid volvulus), prior abdominal surgery.
Main Etiology
Colorectal cancer (~60%); sigmoid volvulus (~15%); colonic pseudo-obstruction (Ogilvie's)
Diverticular stricture; cecal volvulus (younger patients — true emergency); extrinsic compression
Most Common DDx
Small bowel obstruction (dilated small bowel loops predominant; no colonic gas distal to obstruction; step-ladder pattern; adhesion history more likely)
Ogilvie's syndrome (colonic pseudo-obstruction — massive colon dilation but no mechanical cause on CT; no transition point; immobility + narcotics + metabolic precipitants; treat with neostigmine)
Sigmoid volvulus (coffee bean sign on AXR; bird's beak on CT; decompressible with sigmoidoscopy; recurrence high without surgery)
Cecal volvulus (younger patient; right-sided distension; CT shows cecum displaced to left upper quadrant; surgical — NOT reliably decompressible endoscopically)
Toxic megacolon in IBD/C. diff (colonic dilation + systemic toxicity; fever + tachycardia; not true mechanical obstruction but colonic dilatation requiring urgent treatment)
Diverticulitis with localized ileus (LLQ mass effect; CT shows pericolic stranding; fever; WBC elevated; no complete obstruction)
DATA
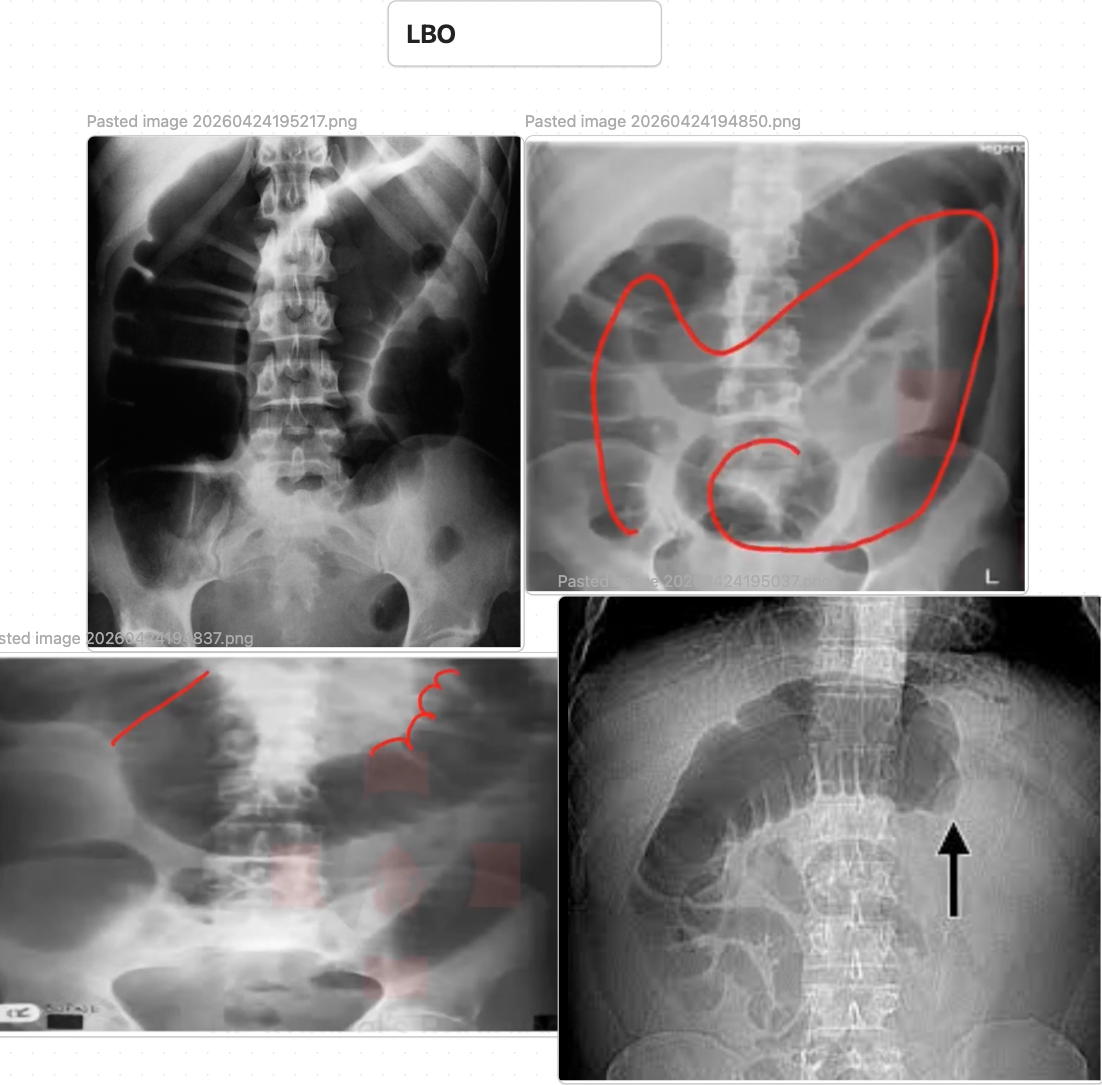
CBC, BMP, lactate; AXR (massively dilated colon; cecal diameter >12 cm = perforation risk; coffee bean sign in sigmoid volvulus)
CT abdomen/pelvis (gold standard — bird's beak transition; identifies cause, ischemia, perforation)
Flexible sigmoidoscopy (therapeutic for sigmoid volvulus)
Home Meds
Opioids, anticholinergics (worsen — hold); anticoagulants (hold if surgery anticipated)
Plan
NPO; IV fluid resuscitation; NGT decompression; Foley; surgery consult immediately
Malignant LBO: SEMS (self-expanding metallic stent) as bridge to surgery or palliation; Hartmann's procedure or primary anastomosis + diverting ileostomy; oncology + surgery + GI multidisciplinary
Sigmoid volvulus: Flexible sigmoidoscopy + rectal tube decompression (first-line if no peritonitis); leave rectal tube 24–48h; elective sigmoid resection before discharge (recurrence ~50–90% without surgery)
Cecal volvulus: Urgent surgery (high ischemia risk; endoscopic not reliable)
Ogilvie's syndrome: Correct underlying cause (metabolic, reduce narcotics); Neostigmine 2 mg IV over 3–5 min if cecal diameter >12 cm (cardiac monitor + atropine at bedside); colonoscopic decompression if neostigmine fails
Serial abdominal exams; cecal diameter monitoring; daily CBC, BMP, lactate; trend fever curve
GI + surgery + oncology consults; PT/OT perioperatively
Discharge: Surgery follow-up 2 weeks; oncology for malignant LBO; stoma education if ostomy placed; elective sigmoid resection scheduling for volvulus
Red Flags
Cecal diameter >12 cm → imminent perforation → urgent intervention
Pneumoperitoneum → free perforation → emergent surgery
Peritoneal signs → ischemia or perforation → emergent surgery
Cecal volvulus → urgent surgery (cannot be reliably managed endoscopically)
Failed endoscopic decompression of sigmoid volvulus → surgery
Senior IM Resident Pearls
Ogilvie's: Neostigmine 80–90% effective; requires cardiac monitoring; absolute contraindication in mechanical obstruction — always confirm no mechanical cause on CT first
Coffee bean sign = sigmoid volvulus (omega loop); bird's beak on CT = transition point of volvulus
SEMS vs. surgery for malignant LBO: Stent preferred as bridge (reduces stoma rate) or palliation; not ideal if perforation risk is high
Common mistake: Neostigmine without cardiac monitor or atropine at bedside — severe bradycardia and bronchospasm can occur
Ileus
Functional non-mechanical bowel dysmotility — most commonly postoperative
Symptoms / Associated Sx
Abdominal distension, bloating, nausea, vomiting
Absent or hypoactive bowel sounds
Failure to pass gas or stool after surgery; diffuse non-crampy discomfort
Denies
Colicky pain (rules out mechanical obstruction; ileus pain is dull/non-colicky)
Fever (rules out primary infectious cause — ileus itself may cause low-grade fever)
Peritoneal signs (rules out anastomotic leak or perforation)
Social History (SHx)
Recent surgery (most common), opioids, critical illness, electrolyte disturbance, hypothyroidism, retroperitoneal process.
Main Etiology
Postoperative ileus (normal physiologic ≤5 days; >5 days = prolonged)
Opioid-induced bowel dysfunction; metabolic (hypokalemia, hypomagnesemia, hypothyroidism)
Intra-abdominal inflammation (pancreatitis, peritonitis); retroperitoneal pathology; medications (anticholinergics, CCBs)
Most Common DDx
Mechanical small bowel obstruction (colicky pain vs. non-crampy; step-ladder pattern on AXR; transition point on CT; no gas throughout colon; gastrografin challenge helps differentiate)
Anastomotic leak (post-surgical ileus >5 days + fever + leukocytosis + tachycardia; CT shows extraluminal air/fluid or abscess — emergent surgical emergency)
Intra-abdominal abscess (fever + localized tenderness + ileus post-operatively; CT shows collection; requires drainage)
Ogilvie's syndrome (massive colonic dilation; immobility + narcotics; cecal diameter >12 cm; neostigmine or colonoscopic decompression)
Hypokalemia-induced bowel dysfunction (K+ <3.0; AXR shows diffuse gas; electrolyte repletion resolves it rapidly)
Hypothyroidism (prolonged ileus + constipation; TSH elevated; resolves with thyroid hormone replacement)
DATA
BMP (hypokalemia, hypomagnesemia — critical; creatinine); CBC (leukocytosis — secondary infection)
Thyroid function (if prolonged or unclear); AXR (diffuse bowel gas throughout small + large bowel; no transition point)
CT abdomen (if prolonged or atypical — rule out mechanical cause, abscess, anastomotic leak)
Home Meds
Opioids (primary contributor — reduce dose or switch to non-opioid); anticholinergics (hold); CCBs (reduce motility — note)
Plan
Identify and correct underlying cause (electrolytes, reduce opioids, treat intra-abdominal source)
NPO until BF returns; IV fluid resuscitation; NGT if significant nausea/distension
Electrolyte repletion (most important): K+ to >4.0; Mg2+ to >2.0
Early ambulation — single most effective intervention for post-op ileus
Minimize opioids; multimodal analgesia (ketorolac, acetaminophen, regional blocks)
Alvimopan (Entereg) 12 mg PO BID — FDA-approved for post-operative ileus (bowel surgery); start pre-op, continue ≤7 days
Methylnaltrexone (Relistor) 8 mg SQ — opioid-induced constipation/ileus in non-surgical patients; does not cross BBB (preserves analgesia)
Chewing gum (modest benefit — stimulates cephalic vagal response)
Daily BMP; repeat KUB if distension worsening; surgery consult if prolonged (>5 days); PT/OT; early ambulation protocol
Discharge: Low-residue diet advancing to regular; stool softeners (docusate sodium 100 mg BID) with any opioid; minimize opioids; activity as tolerated
Red Flags
Ileus >5–7 days post-op + worsening distension → CT to rule out abscess, anastomotic leak, or mechanical obstruction
Fever + leukocytosis + ileus → intra-abdominal sepsis/anastomotic leak → CT + surgery immediately
Cecal dilation >12 cm → Ogilvie's protocol or surgery
K+ <3.0 refractory to repletion → aggressive IV replacement; cardiac monitoring
Senior IM Resident Pearls
Hypokalemia is the most reversible cause of ileus — always normalize K+ (>4.0) before attributing to post-op state
Alvimopan: Hospital-restricted; max 15 doses; cannot use in patients on opioids >7 days (rebound effect)
Early ambulation > any pharmacologic intervention — enforce walking as priority in post-op ileus
Common mistake: Continuing full opioid dose without non-opioid adjuncts — ketorolac + acetaminophen + regional anesthesia significantly reduce ileus duration
Bowel Perforation
Full-thickness bowel wall disruption — surgical emergency; medicine manages pre-operative optimization and co-management
Symptoms / Associated Sx
Sudden-onset severe abdominal pain (often "worst of life")
Rigid, board-like abdomen (peritonitis); rebound tenderness, guarding
Fever, tachycardia, hypotension (sepsis/septic shock)
Referred shoulder pain (diaphragmatic irritation from free air)
Denies
Gradual onset pain (rules out perforation as diagnosis — acute onset is defining feature)
Steroid/NSAID use (these mask peritoneal signs — do not be reassured by absence if on steroids)
Social History (SHx)
Prior PUD, IBD, diverticulitis, colon cancer, recent colonoscopy/ERCP, foreign body, trauma, steroid/NSAID use (mask symptoms), immunosuppression.
Main Etiology
Perforated peptic ulcer (anterior duodenal or gastric — most common non-traumatic)
Diverticular perforation (Hinchey III–IV); colorectal cancer (obstructing or perforating)
IBD (toxic megacolon, transmural); ischemic bowel (necrosis)
Iatrogenic: colonoscopy, ERCP, NGT/Dobhoff malposition; foreign body; trauma
Most Common DDx
Acute mesenteric ischemia (severe pain out of proportion to exam; vascular risk factors; lactate elevated; CT angiography shows mesenteric vessel occlusion; free air usually absent initially)
Ruptured abdominal aortic aneurysm (sudden severe abdominal/back pain; pulsatile abdominal mass; hemodynamic instability; CT aortography; no free air in bowel)
Severe pancreatitis (epigastric pain radiating to back; lipase >3× ULN; peripancreatic fluid on CT; free air usually absent)
Diverticulitis without free perforation (Hinchey I–II; no free air; pericolonic abscess; can be managed non-operatively)
Spontaneous bacterial peritonitis (SBP) (cirrhotic + ascites + PMN ≥250; no free air; no mechanical cause; treat with antibiotics not surgery)
Post-procedural pain (endoscopy-related discomfort — important to image and rule out perforation before attributing to gas pain)
DATA
CBC, BMP, lactate, blood cultures × 2, PT/INR, type and crossmatch
AXR upright (free air under diaphragm — 70–80% sensitivity); CT abdomen/pelvis with IV contrast (gold standard — free air, free fluid, wall defect; 95% sensitive)
Home Meds
NSAIDs, corticosteroids (mask symptoms — note prior use); anticoagulants (reverse pre-operatively)
Plan
Surgical emergency — surgery consult in parallel with stabilization
NPO; 2 large-bore IVs; aggressive IVF; Foley; pain management (do not withhold — evidence shows analgesia does not mask surgical findings)
NGT decompression; pre-operative optimization (correct coagulopathy/electrolytes; notify anesthesia)
Antibiotics immediately (source control pending):
Community-acquired: Piperacillin-tazobactam 3.375 g IV q6h
Healthcare-associated/severe sepsis: Meropenem 1 g IV q8h ± Vancomycin
Duration: 4–5 days post-operative if source controlled
Vasopressors (norepinephrine) if septic shock unresponsive to 30 mL/kg IVF → ICU
Surgical options by etiology:
Perforated duodenal ulcer: Graham patch repair
Perforated gastric ulcer: patch + biopsy (rule out malignancy)
Perforated diverticulitis: Hartmann's or primary anastomosis + diverting ileostomy
Colorectal cancer: resection ± ostomy; ischemic bowel: necrotic segment resection
ICU post-operatively; daily CBC, BMP, lactate; trend fever curve; PT/OT; early mobilization
Discharge: Wound care; PPI ongoing if PUD-related; H. pylori treatment; oncology if malignancy-related; surgery follow-up 2 weeks
Red Flags
Free air on imaging → surgical emergency → immediate surgery; do not delay for further workup
Septic shock (MAP <65 despite fluids) → vasopressors + ICU + emergent source control
Lactate >4 → mortality increases with every hour delay to source control
Steroid use + perforation → peritoneal signs may be absent; maintain high suspicion
Post-colonoscopy pain + distension → perforation until proven otherwise → CT immediately
Senior IM Resident Pearls
Free air on upright CXR = pneumoperitoneum (if no recent surgery) — 70–80% sensitivity; CT is 95% sensitive
Steroids and NSAIDs mask peritoneal signs — always CT and examine carefully in patients on chronic steroids; absence of guarding does not rule out perforation
Withholding analgesia for "surgical abdomen" is outdated — multiple RCTs show opioids do not impair surgical decision-making; pain relief is appropriate and humane
Common mistake: Attributing post-colonoscopy pain to "gas pain" without imaging — rule out perforation with CT for any significant post-procedure pain