Acute Kidney Injury
Rhabdomyolysis
Skeletal muscle breakdown releasing myoglobin and intracellular contents
CK >5 times the upper limit of normal (typically >1,000 U/L), (intrarenal) AKI, specifically acute tubular necrosis (ATN) from myoglobin‑mediated tubular injury and renal ischemia
SYMPTOMS / ASSOCIATED SX
Classic triad (only ~10% have all three): myalgias + weakness + dark (tea/cola-colored) urine
Muscle swelling, tenderness, rigidity; focal compartment firmness
Oliguria, AKI symptoms (nausea, fatigue, edema)
Severe: cardiac arrhythmias (hyperkalemia), seizures (hypoNa/hypoCa), DIC
History: found down, crush injury, seizure, extreme exertion, drug/alcohol use, heat stroke
DENIES
Recent statin initiation or dose increase (drug-induced)
Chest pain/ischemic symptoms (MI can cause mild CK elevation — rule out if troponin elevated)
Seizure activity (seizure-induced rhabdo)
Extreme heat or prolonged exercise (exertional rhabdo)
SOCIAL HISTORY
Alcohol (direct myotoxin + falls + prolonged immobility); stimulant use (cocaine, MDMA); statin use
Recent extreme exercise, military training, heat exposure, prolonged immobilization
MAIN ETIOLOGY
Traumatic/compressive: crush injury, prolonged immobilization ("found down"), compartment syndrome
Exertional: extreme exercise, heat stroke, seizures
Toxic: alcohol (most common), statins (especially with CYP3A4 inhibitors), cocaine, MDMA, colchicine, NMS
Infectious: viral myositis (influenza, COVID-19), bacterial sepsis
Metabolic: hypothyroidism, hypokalemia, hypophosphatemia; inflammatory: polymyositis/dermatomyositis
MOST COMMON DDX
AKI from other causes (pigmented casts = rhabdo; coarse granular = ATN)
MI (troponin elevated but CK-MB fraction <5% of total CK in rhabdo; ECG)
NMS (antipsychotic use, fever, rigidity, AMS — CK often >1000)
Malignant hyperthermia (inhalational anesthetic/succinylcholine — RYR1 mutation)
Serotonin syndrome (serotonergic drugs, hyperreflexia, clonus, agitation)
Inflammatory myopathy (subacute, skin changes, autoimmune markers)
DATA
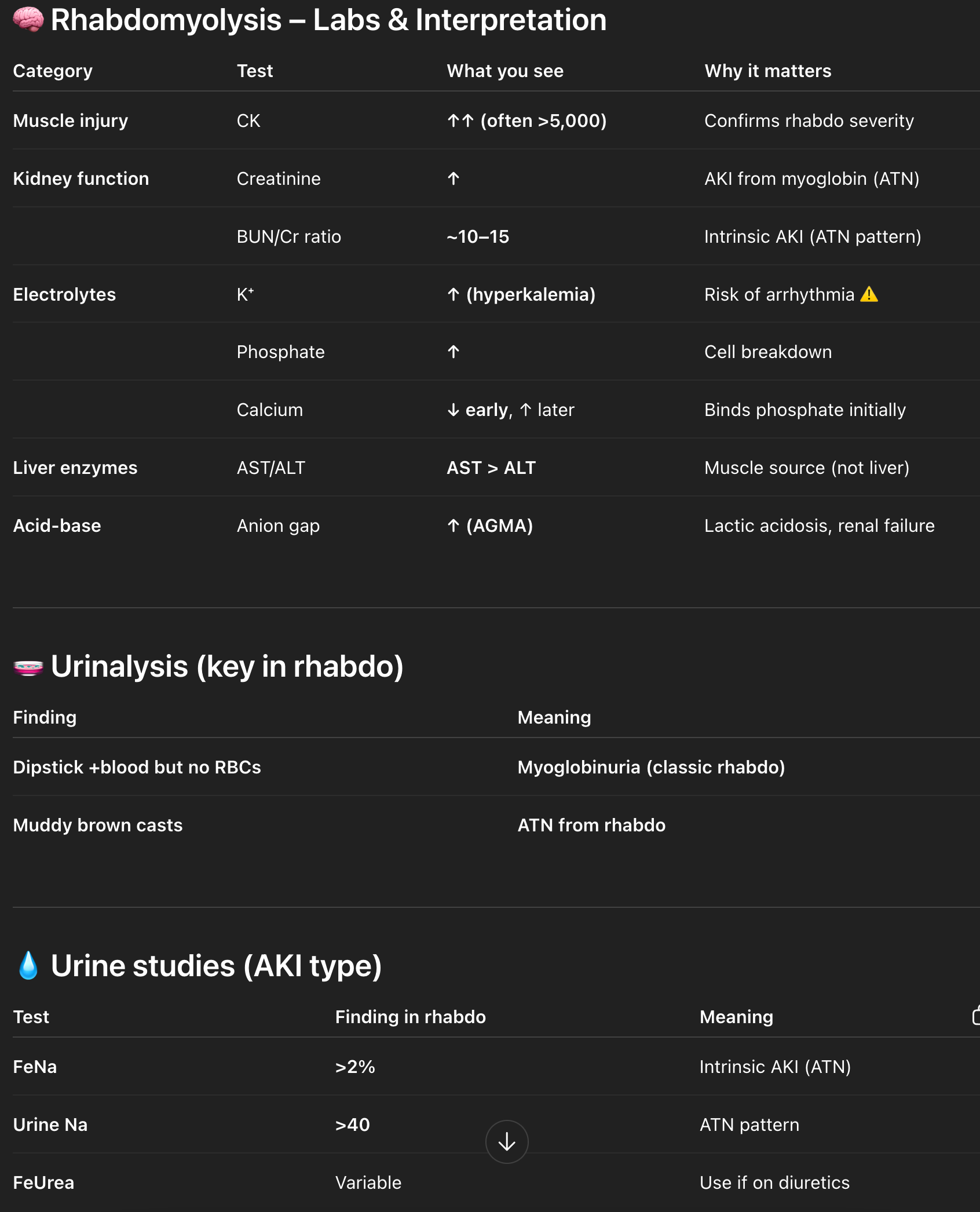
Baseline BUN/Cr: BUN:Cr 10–15 suggests intrinsic AKI (e.g., ATN from rhabdomyolysis)
CBC
BMP: monitor for HyperK, HyperPhos, HyperCa
CK: elevated; trend daily
LFTs:AST > ALT with normal ALK Phos supports muscle injury over hepatic source
Anion Gap: elevated AGMA common
Urinalysis (UA):
Myoglobinuria: positive blood with <3 RBCs/hpf
Hyaline casts → pre-renal AKI
Muddy brown casts → ATN
RBC casts → glomerulonephritis
WBC casts → acute interstitial nephritis
Urine Studies:
FeNa <1% → pre-renal
FeNa >2% → ATN
Less reliable in CKD
FEUrea <35% → pre-renal (especially if on diuretics)
Urine Na <20 → pre-renal
Urine Na >40 → ATN
Urine Creatinine
Imaging:
Renal US if concern for obstruction
CT A/P if obstruction not adequately evaluated or alternate intra-abdominal pathology suspected
HOME MEDS
Statins — HOLD immediately; do not restart until CK normalized and etiology investigated
Fibrates — hold (potentiate statin myopathy)
ACE inhibitors/ARBs, NSAIDs — hold if AKI
K-sparing diuretics — hold (hyperkalemia risk)
PLAN
Fluid Resuscitation (Cornerstone)
LR 1–2 L IV bolus initially → then LR 200–500 mL/hr continuous
Adjust fluids to urine output goal 200–300 mL/hr
Continue until:
CK downtrending (<5,000 U/L in most guidelines)
Cr stable or improving
No ongoing myoglobinuria
Electrolytes normalized
Monitor for Volume Overload
Daily assessment for pulmonary edema
Daily weights
Strict I/O
Stop or reduce fluids if:
Pulmonary edema develops
3–5 L positive fluid balance
Significant volume overload (regardless of CK)
AKI Workup / Monitoring
Follow FeNa or FEUrea
Follow Urine Na (>40 ATN; <20 pre-renal)
Follow Urine Creatinine
Trend BMP q12h initially, then daily
Daily BUN/Cr
Daily CK
Electrolytes
Monitor and replete electrolytes as needed
Closely monitor:
Hyperkalemia
Hyperphosphatemia
Hypercalcemia
AGMA
Medication Management
Hold nephrotoxins
Hold home ACEi/ARB
Hold diuretics
Monitoring
Telemetry
Strict I/O
Daily weights
Nephrology consult early for CK >10,000, AKI, or refractory electrolytes
DISCHARGE:
CK trending down (ideally <1000) and renal function stable before discharge
HMGCR antibody if statin myopathy not resolving after stopping statin (IMNM)
Nephrology follow-up if AKI occurred; PCP 1–2 weeks
Metabolic workup if recurrent exertional rhabdo (McArdle's, carnitine deficiency)
RED FLAGS
Hyperkalemia >6.0 + ECG changes → calcium gluconate immediately + insulin/dextrose + emergent dialysis
Oliguria unresponsive to >6–10 L IVF → ATN/oliguric AKI; early dialysis
Compartment syndrome: 6 P's — Pain, Pressure, Paresthesia, Pallor, Pulselessness, Paralysis (late); pressure >30 mmHg = surgical emergency
CK >50,000 → extremely high AKI risk; aggressive resuscitation + bedside nephrology
DIC → hematology; FFP/cryoprecipitate as needed
MH: temperature >40°C + rigidity after anesthesia → dantrolene 2.5 mg/kg IV; cool aggressively; ICU
SENIOR IM RESIDENT PEARLS
Classic triad present in only ~10% — diagnose biochemically; always check CK in "found down" patients
Hypocalcemia in rhabdo: DO NOT treat asymptomatically — calcium deposits in muscle reabsorb during recovery → rebound hypercalcemia
Statin + CYP3A4 inhibitor (azithromycin, diltiazem, fluconazole, grapefruit) dramatically increases myopathy risk
FeNa <1% early in rhabdo AKI because still prerenal — start fluids immediately, do not wait
Common mistake: under-resuscitating rhabdo — patients often need 10+ L in first 24h; track urine output hourly
HMGCR Ab-positive IMNM: does NOT resolve after stopping statin; requires prednisone + immunosuppression
Bicarbonate alkalinization: target urine pH >6.5; avoid if HCO3 >30 or pH >7.5; monitor q2–4h