Acute Hypoxic Respiratory Failure
Pulmonary Embolism
-Symptoms / Associated Sx
Acute onset dyspnea (most common symptom)
Pleuritic chest pain (peripheral PE with infarction)
Tachycardia, tachypnea, hypoxia
Hemoptysis (pulmonary infarction — late finding)
Syncope or presyncope (massive PE — obstructive shock)
Leg pain, swelling, erythema (concomitant DVT in ~50%)
Hypotension, diaphoresis, altered mentation (massive PE — RV failure)
Denies
Fever + productive cough + focal consolidation (rules out pneumonia as primary)
Bilateral leg edema + JVD + elevated BNP (rules out CHF as primary)
Recent immobility, surgery, malignancy, OCP, prior VTE (reduces PE likelihood if truly absent)
Normal D-dimer with low pre-test probability (rules out PE — negative predictive value ~99%)
Social History (SHx)
Recent surgery (especially orthopedic, pelvic, abdominal), immobility, malignancy, prior VTE, OCP/HRT, pregnancy/postpartum, long-distance travel, hereditary thrombophilia, obesity, smoking.
Main Etiology
Virchow's triad: stasis + hypercoagulability + endothelial injury
Provoked: surgery, trauma, immobility, OCP/HRT, pregnancy, malignancy
Unprovoked: idiopathic; evaluate for occult malignancy and thrombophilia
Fat embolism (long bone fracture), air embolism, amniotic fluid embolism (obstetric)
Most Common DDx
Pneumonia (fever + consolidation; elevated WBC + procalcitonin; responds to antibiotics; no filling defect on CTPA)
Acute coronary syndrome (chest pain + EKG changes + troponin; bilateral leg edema less; echo shows LV dysfunction vs. RV strain)
Aortic dissection (sudden severe tearing back pain; pulse differential; CT aortography — PE and dissection both cause elevated D-dimer)
CHF / flash pulmonary edema (bilateral symmetric infiltrates; BNP markedly elevated; responds to diuretics; no filling defect on CTPA)
Pericardial tamponade (obstructive shock; JVD + hypotension + muffled heart sounds; echo shows pericardial effusion + RV collapse)
Tension pneumothorax (absent unilateral breath sounds; tracheal deviation; CXR or POCUS confirms)
DATA
Pre-test probability: Wells PE score (≤4 = low-moderate; >4 = high); PERC rule (if all 8 criteria met → PE excluded without D-dimer in low pre-test probability)
D-dimer (use only in low-to-moderate pre-test probability; negative NPV ~99% → PE excluded; age-adjusted D-dimer threshold = age × 10 mcg/L in patients >50)
CT pulmonary angiography (CTPA) — gold standard; first-line imaging; sensitivity ~95%, specificity ~98%
V/Q scan (if contrast contraindicated or renal failure; less specific with parenchymal disease)
EKG (sinus tachycardia most common; S1Q3T3 pattern — only 10–20%; T-wave inversions V1–V4 + new RBBB = right heart strain)
Troponin + BNP/NT-proBNP (RV injury markers — elevated = submassive/massive; predicts worse outcome)
Echo (RV dilation, McConnell's sign, D-shaped interventricular septum, elevated RV:LV ratio >0.9)
CBC, BMP, PT/INR, PTT (pre-anticoagulation baseline)
Bilateral lower extremity Doppler US (DVT confirmation — present in ~50%)
Thrombophilia workup (draw BEFORE anticoagulation; defer to outpatient if stable)
Home Meds
Prior anticoagulation (assess compliance — PE on therapeutic anticoagulation → cancer, HIT, antiphospholipid)
OCP/HRT (hold — thrombogenic)
Aspirin (does not prevent VTE adequately)
Plan (Pulmonary Embolism Add-On)
UFH (unstable/massive, possible tPA, thrombectomy, CrCl <30 or unpredictable course) (80/kg/per pharmacy) vs LMWH (Stable / floor / good kidneys) (1.5/kg/per pharmacy )
Apixaban 10mg BID for 7 days followed by 5mg BID (alternative -> for Rivaroxaban 15mg BID for 21 days followed by 20mg daily with dinner ) once stabilized with plan to treat for 3-6 months if provoked or indefinitely if unprovoked/recurrent PE. consider warfrin if Mechanical heart valve,Antiphospholipid Syndrome, or CrCl < 30
Fluid: can begin with 500cc bolus if e/o hypotension, careful not to overload RV
Supplemental O2: target SpO2 ≥92%; avoid aggressive fluid resuscitation (worsens RV dilation + septal shift)
Vasopressors (norepinephrine preferred) if massive PE + hypotension; avoid excessive fluids
IVC filter: only if absolute contraindication to anticoagulation + active bleeding; retrieve when anticoagulation resumes
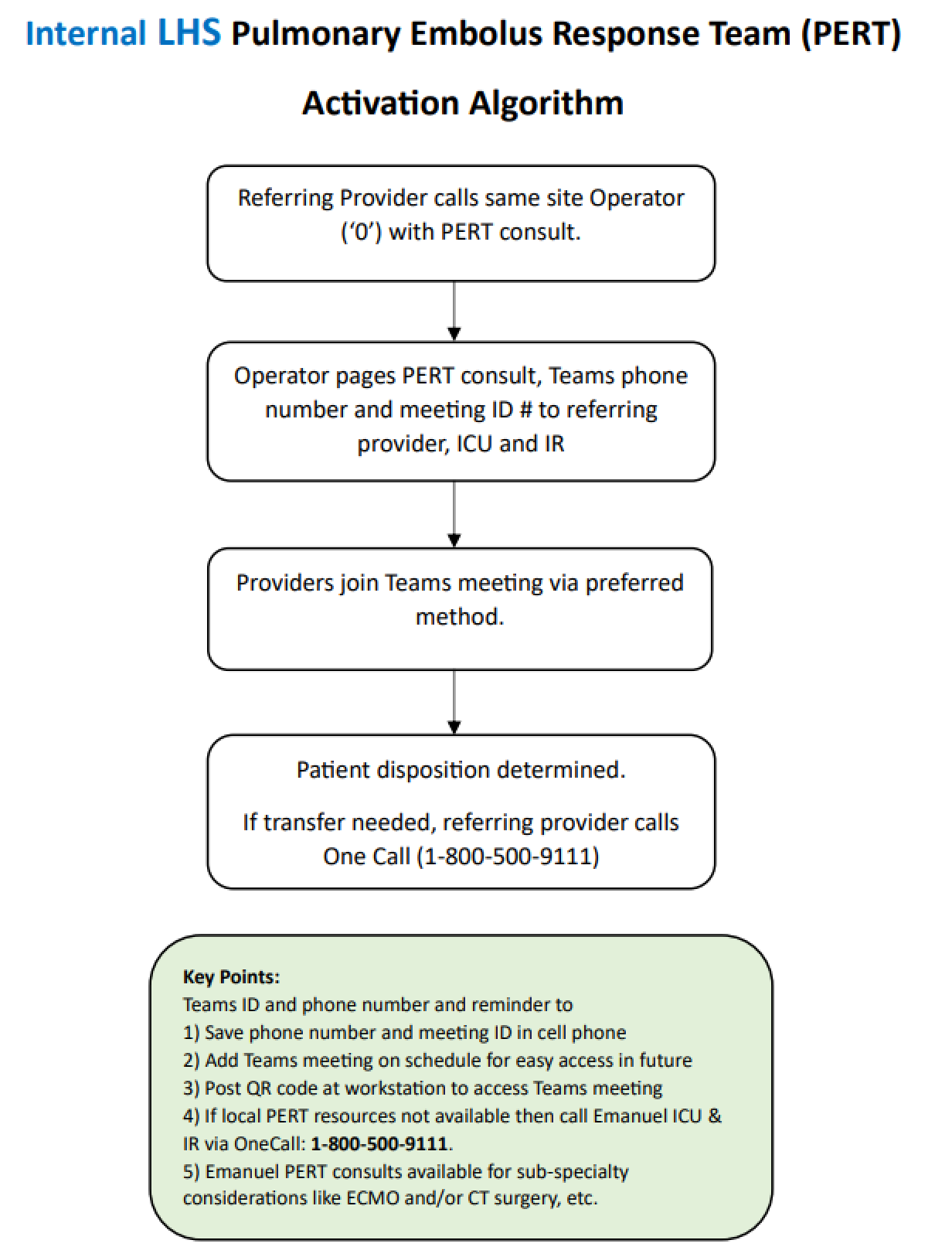
PERT consult for massive/submassive PE
Duration of anticoagulation: Provoked reversible risk factor → 3 months; unprovoked → ≥3 months, discuss extended; cancer-associated → indefinite while cancer active; recurrent unprovoked → indefinite
Trend CBC, BMP, troponin, BNP q12–24h in submassive/massive; serial echo if RV strain
PT/OT; graduated compression stockings; ambulation when stabilized
Discharge: DOAC with clear duration; INR monitoring if warfarin; hold OCP/HRT; malignancy workup if unprovoked; thrombophilia testing 3 months after anticoagulation if unprovoked; hematology/pulmonology follow-up; Homan's sign — patient education on VTE recurrence signs
Advanced Therapy Options if needed
consult ICU/Cards for Systemic thrombolysis (tPA)immediately in unstable patients or massive PE —no fixed time window
consult IR for Catheter-directed therapy (lytics OR Thrombectomy) if tPA contraindicated OR failed or no improvement after 24-48 hr initial therapy
VA-ECMO when Refractory shock / cardiac arrest or Bridge to thrombectomy
Red Flags
SBP <90 + confirmed PE → massive PE → systemic tPA vs. CDT vs. surgical embolectomy; ICU immediately
Cardiac arrest from PE → tPA during CPR; extended CPR (60–90 min) to allow tPA effect
RV:LV ratio >0.9 + hemodynamic stability + rising troponin → submassive PE deteriorating → escalate to CDT or tPA
PE in pregnancy → LMWH only (DOACs and warfarin contraindicated); CTPA preferred if CXR abnormal; MFM + IR consult
PE on therapeutic anticoagulation → CTPA to confirm; consider HIT, APS, malignancy, DOAC non-adherence, subtherapeutic dosing
Senior IM Resident Pearls
PERC rule: 8 criteria — if ALL met in low pre-test probability → PE excluded without D-dimer (age <50, HR <100, SpO2 ≥95%, no leg swelling, no hemoptysis, no prior VTE, no recent surgery/trauma, no OCP/HRT)
Age-adjusted D-dimer (age × 10 mcg/L) in patients >50 — improves specificity without losing sensitivity; reduces unnecessary CTAPAs
McConnell's sign on echo (RV free wall hypokinesis with preserved apex) — highly specific for acute PE; also seen in RV infarction
Fluid bolus in massive PE can WORSEN outcomes by overdistending RV and pushing the interventricular septum leftward (D-sign) — give conservative fluids (250–500 mL max); use vasopressors early
PERT teams reduce escalation time and improve outcomes in submassive/massive PE — activate early in high-risk cases
Common mistake: High-dose D-dimer in high pre-test probability — D-dimer is only a rule-out test in low-moderate probability; never use in high probability patients; go straight to CTPA
Common mistake: Aggressive IV fluids in massive PE — RV is preload-sensitive but only to a point; excess fluid causes RV dilation → septal bowing → LV compression → cardiogenic shock
PE Risk Stratification
Massive PE (High Risk)
→ PE with hemodynamic instability:SBP < 90 mmHg ≥ 15 min OR need for pressors
Cardiac arrest / pulselessness
Severe bradycardia (< 40 bpm) with instability
Submassive PE (Intermediate Risk)
→ PE with normal BP (SBP ≥ 90) BUT evidence of strain:Right ventricular dysfunction (RVD) (echo/CT) and/or
Positive biomarkers (↑ troponin, ± BNP)
Low-Risk PE
→ PE without:Hypotension
RVD
Elevated cardiac biomarkers
Absolute Contraindications for tPA
Active serious bleed
Any history of hemorrhagic CVA
Ischemic CVA in last 3 monhs
Known AVM
Recent brain/spinal surgery
Head trauma with fracture or brain injury in last 3 weeks
Suspected or known aortic dissection
Relative Contraindications for tPA (not exhaustive):
CNS tumor
Major non-CNS surgery in last 2-3 weeks
Ischemic CVA > 3 months ago
plt <100, INR >1.7, fibrinogen <150
Use of oral AC in last 48 hours
GI bleed in last month
BP >180/110
Age >75 yo
Advanced cirrhosis (coagulopathy)