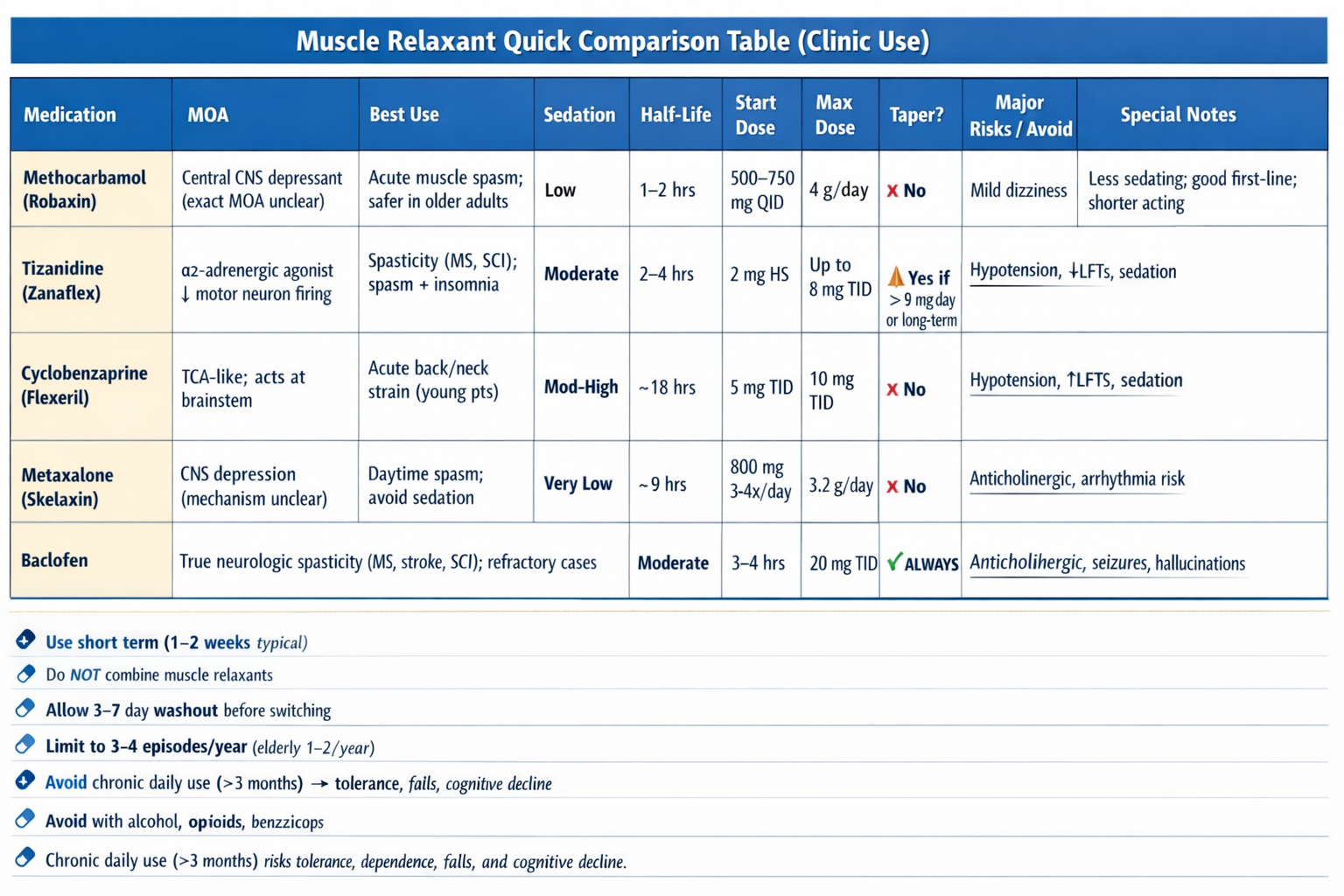
Methocarbamol (Robaxin)
(half-life 1–2 hours)
Mechanism unclear, likely CNS depressant. Less sedating than cyclobenzaprine and associated with decreased hospital length of stay in trauma patients with rib fractures.
Indication: Acute muscle spasm
Choose when: Want less sedation, safer in older adults
Start: 500–750 mg PO QID
Max: 4 g/day
Taper not needed
With or without food (take with food if stomach upset)
Tizanidine (Zanaflex)
(half-life 2–4 hours) (1–3 weeks; titrate; moderate sedation)
Alpha-2 adrenergic agonist that reduces spasticity by increasing presynaptic inhibition of motor neurons. Sedative properties may benefit patients with insomnia from muscle spasms.
Indication: Spasticity (MS, spinal cord injury), sometimes muscle spasm
Watch for: Hypotension, sedation, ↑ LFTs
Start: 2 mg PO at bedtime
Increase by 2–4 mg every 3–7 days as needed
If needed, up to 8 mg TID
Taper if >9 mg/day or long-term use
Decrease gradually over 1–2 weeks
With or without food (take with food if stomach upset)
Cyclobenzaprine (Flexeril)
(half-life ~18 hours) (nighttime only; moderate–high sedation)
Structurally similar to tricyclic antidepressants; acts on the brainstem to reduce tonic somatic motor activity.
Indication: Acute back/neck spasm
For young patients with acute muscle spasm
Avoid in: Elderly (anticholinergic effects), arrhythmia, glaucoma
Start: 5 mg PO TID
Titrate: Increase to 10 mg TID if needed
Duration: Short term (≤2–3 weeks)
Taper not needed
With or without food (take with food if stomach upset)
Metaxalone (Skelaxin)
(least sedating)
Short-term (1–2 weeks), ideal for daytime use.
Dosage: 800 mg PO 3–4 times/day (max 3.2 g/day)
Take with food to reduce GI upset
Higher cost and less generic availability, but increasingly used when sedation avoidance is prioritized
(MOA) remains incompletely understood but is attributed to general CNS depression
Baclofen
(half-life 3–4 hours) (2–4 weeks; taper)
GABA-B receptor agonist. More commonly used for spasticity from upper motor neuron syndromes but also indicated for musculoskeletal conditions; more for refractory cases.
Indication: Spasticity (MS, stroke, SCI)
Choose when: True neurologic spasticity
Warning: Abrupt discontinuation → seizures
ALWAYS taper over 1–2 weeks to avoid seizures, hallucinations, rebound spasticity
Start: 5 mg PO TID
Increase by 5 mg every 3 days as needed up to 20 mg TID
With or without food (take with food if stomach upset)
Notes
If one muscle relaxant fails after a full short-term course (e.g., 1–2 weeks), you can safely switch to another.
Complete the course + 3–7 day break to clear the drug and avoid overlapping sedation.
Try to limit to 3–4 discrete episodes per year.
Never overlap or combine due to additive CNS depression; elderly patients: max 1–2 episodes/year.
These medications are used for acute flares.
Chronic daily use (>3 months) risks tolerance, dependence, falls, and cognitive decline.
Quick Guide
Indication: Acute muscle spasm (short-term use only 1–2 weeks).
Selection:
- Older adult → Methocarbamol or Metaxalone
- Needs daytime function → Metaxalone
- Spasm + insomnia → Tizanidine (night)
- Young acute strain → Cyclobenzaprine (short term)
- True neurologic spasticity → Baclofen
Dosing:
- Methocarbamol 500–750 mg QID (max 4 g/day)
- Tizanidine 2 mg HS → titrate (monitor BP/LFTs)
- Cyclobenzaprine 5 mg TID → 10 mg TID if needed
- Metaxalone 800 mg 3–4x/day
- Baclofen 5 mg TID → titrate (ALWAYS taper)
Safety:
- Do NOT combine muscle relaxants
- Avoid alcohol, opioids, benzos
- Limit to ≤3–4 episodes/year (elderly ≤2/year)
- Avoid chronic daily use (>3 months)