Acute respiratory failure with Hypoxia and Hypercarbia
COPD exacerbation
Symptoms / Associated Sx
Increased dyspnea (beyond baseline), worsening cough
Increased sputum production or change in sputum color (purulent = bacterial trigger)
Wheezing, chest tightness, accessory muscle use
Hypoxia (SpO2 below patient's baseline), tachypnea, tachycardia
Hypercapnia with altered mentation (respiratory acidosis — severe)
Pursed-lip breathing, barrel chest, hyperresonance on percussion (exam)
Denies
Fever + productive cough + focal consolidation (rules out pneumonia as the primary trigger if absent — though may coexist)
Orthopnea, PND, bilateral leg edema (rules out CHF as primary cause of dyspnea)
Pleuritic chest pain + unilateral absence of breath sounds (rules out pneumothorax)
New onset in non-smoker without prior diagnosis (raises alternative diagnoses)
Social History (SHx)
Smoking history (pack-years; current vs. former), occupational exposures (dust, fumes, coal), home oxygen use, prior COPD exacerbations and hospitalizations (frequency predicts future risk), inhaler types and compliance, prior intubations, baseline exercise tolerance and SpO2.
Main Etiology
Viral URI (~50%) — rhinovirus most common; influenza, RSV, parainfluenza
Bacterial (~25%) — Haemophilus influenzae, Moraxella catarrhalis, Streptococcus pneumoniae; Pseudomonas in severe COPD (FEV1 <30%, frequent exacerbations, bronchiectasis)
Environmental triggers — air pollution, cold air, smoke exposure
Medication noncompliance (missed inhalers)
No identifiable cause (~25%)
Most Common DDx
Acute decompensated heart failure (bilateral crackles + JVD + leg edema + elevated BNP; CXR shows bilateral infiltrates + cardiomegaly; responds to diuresis not bronchodilators)
Community-acquired pneumonia (fever + focal consolidation on CXR; elevated WBC/procalcitonin; more than typical COPD sputum change)
Pulmonary embolism (acute dyspnea + hypoxia; tachycardia; pleuritic chest pain; D-dimer + CTPA; no wheezing; Wells score)
Pneumothorax (sudden onset dyspnea; decreased unilateral breath sounds; tracheal deviation; CXR confirms)
Asthma exacerbation (younger patient; atopy; no smoking history; fully reversible obstruction; no emphysematous changes on imaging)
Acute respiratory failure from non-COPD cause — ACS with flash pulmonary edema (chest pain + EKG changes + troponin; does not wheeze)
DATA
ABG (pH, PaCO2, PaO2 — respiratory acidosis in hypercapnic failure; baseline hypercapnia common in severe COPD)
SpO2 and titrated O2 (target SpO2 88–92% — avoid hyperoxia causing hypercapnia in CO2 retainers)
CBC (leukocytosis → bacterial trigger)
BMP (electrolytes — hypokalemia from beta-agonists; creatinine)
BNP/NT-proBNP (rule out CHF)
Procalcitonin (guides antibiotic use — >0.1 ng/mL supports bacterial etiology)
CXR (infiltrate → pneumonia; hyperinflation, flattened diaphragms; exclude pneumothorax)
EKG (cor pulmonale — right heart strain; p-pulmonale; multifocal atrial tachycardia in COPD)
Sputum culture (if purulent and hospitalized; guides antibiotic narrowing)
Viral respiratory panel (influenza, RSV, COVID-19)
Spirometry (not during acute exacerbation — defer to outpatient)
Home Meds
SABA (albuterol), SAMA (ipratropium), LABA, LAMA, ICS inhalers — assess compliance and technique
Home oxygen (flow rate and hours/day)
Systemic steroids if on chronic prednisone (do not abruptly stop)
Theophylline (narrow therapeutic index; toxicity risk — check level)
Diuretics (if concurrent CHF component)
Plan (COPD add On)
scheduled duonebs q4h / albuterol q2 PRN; space as able,
PO prednisone 40mg for 5 days; If unable to take PO, give methylprednisolone 40 mg IV daily, then transition to prednisone when able.
if infectious trigger suspected -> CTX 1g IV for 5 days , Azithromycin 500mg for three days, (Cefepime 2g (5–7 days) if risk of PsA), On DC Augmentin 875/125 mg BID alone to complete ~5 day
Monitoring daily CBC, BMP, tele
Bronchopulmonary hygeine: PEP/flutter
PT/OT for eval
NicWiPP Protocol ADD-ON
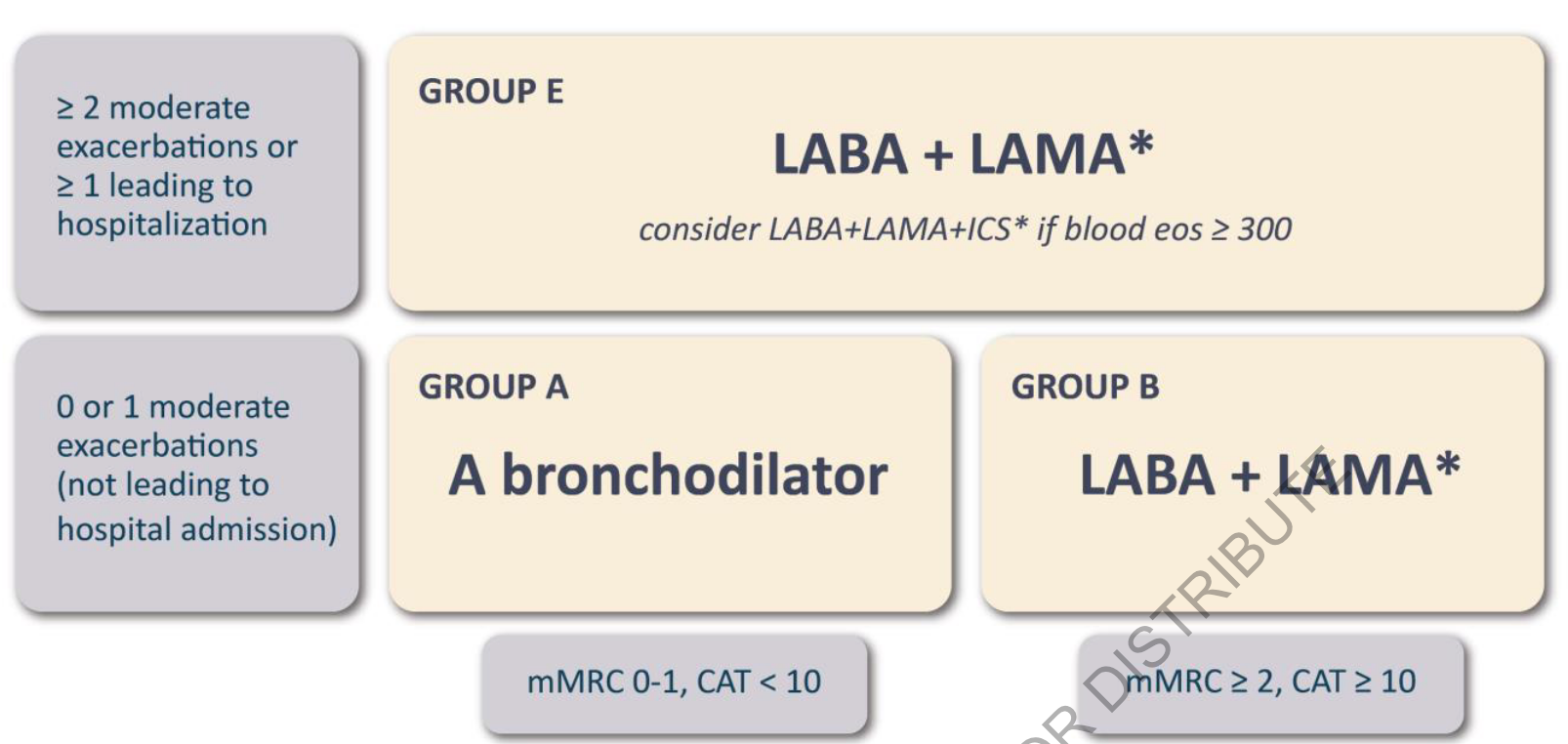
consider Pulm consult if refractory or in need of Roflumilast (FEV1 < 50%) or Dupilumab (Eso>300)
O2 prn to maintain SpO2 88-92%
ambulate with Oxygen order prior to DC
Resume/optimize maintenance inhalers prior to discharge
Smoking cessation counseling
BiPAP/NIPPV if hypercapnia, increased WOB, or respiratory acidosis
VBG PRN for worsening respiratory status
Red Flags
pH <7.30 + PaCO2 >60 + altered mentation → BiPAP immediately; if fails → intubation
Hyperoxia (SpO2 >96%) in COPD → worsens hypercapnia → titrate O2 to 88–92%
Failure to improve on BiPAP at 1–2h (pH not improving, worsening mentation) → intubation urgently
Multifocal atrial tachycardia (MAT) + COPD → hallmark of severe hypoxemia in COPD; treat underlying COPD not arrhythmia with antiarrhythmics
Respiratory arrest or apnea → emergent intubation
Senior IM Resident Pearls
GOLD criteria exacerbation severity: Mild = SABA only; Moderate = SABA + antibiotics ± steroids; Severe = hospitalization or ED visit; Very Severe = ICU admission or acute respiratory failure
Anthonisen criteria for antibiotics: ≥2 of 3 cardinal symptoms (increased dyspnea, increased sputum volume, increased sputum purulence) → antibiotics reduce exacerbation duration and hospitalization
5-day prednisone is equivalent to 14-day course (REDUCE trial) — use the shorter course; reduces steroid side effects without worse outcomes
Hyperoxia causes hypercapnia via Haldane effect (CO2 released from hemoglobin as O2 saturates it) + loss of hypoxic drive; SpO2 target 88–92% is the evidence-based range
MAT (multifocal atrial tachycardia) in COPD — multiple P-wave morphologies; do NOT treat with antiarrhythmics; treat the underlying COPD and hypoxemia; verapamil if symptomatic only
Common mistake: Giving high-flow O2 to COPD patients with hypercapnia — SpO2 >96% drives CO2 retention; titrate carefully to 88–92%
Common mistake: Using corticosteroids for >5 days routinely — REDUCE trial showed non-inferiority of 5-day course; prolonged steroids increase pneumonia risk, hyperglycemia, and muscle wasting
Labs
CBC daily
BMP daily
Mg daily
Phos daily
VBG/ABG on admission
Repeat VBG/ABG PRN worsening respiratory status
BNP/NT-proBNP
Procalcitonin
Respiratory viral panel (COVID/Flu/RSV)
Sputum culture if productive sputum
Blood cultures x2 if febrile/septic
Troponin if chest pain
Imaging
CXR portable
CT Chest if alternative diagnosis suspected
CTA Chest if PE suspected
Respiratory
Supplemental O2 to maintain SpO2 88–92%
Continuous pulse oximetry
Duonebs q4h scheduled
Albuterol nebulizer q2h PRN
Incentive spirometry
PEP/flutter valve therapy
RT consult
Steroids
Prednisone 40 mg PO daily × 5 days
If unable to take PO:
Methylprednisolone 40 mg IV daily
Transition to prednisone when able
Antibiotics
Standard coverage:
Ceftriaxone 1 g IV q24h × 5 days
Azithromycin 500 mg PO/IV daily × 3 days
Pseudomonas risk:
Cefepime 2 g IV q8h × 5–7 days
Discharge:
Augmentin 875/125 mg PO BID to complete ~5 days total
Monitoring
Telemetry
Continuous pulse ox
Vitals q4h
Strict I&O
Daily weights
Trend CBC/BMP daily
Monitor fever curve
BiPAP/NIPPV
Initiate for:
Hypercapnia
Increased WOB
Respiratory acidosis
Persistent hypoxia
Escalate:
pH <7.30
PaCO₂ >60 with worsening mentation
Failed BiPAP after 1–2 hrs
Respiratory arrest/apnea
Consults
RT
PT/OT eval and treat
Case management
Pulmonology PRN
Home Meds
Resume maintenance inhalers
Verify inhaler compliance
Continue home oxygen if indicated
Check theophylline level if applicable
DVT PPX
Enoxaparin 40 mg SQ daily
OR
Heparin 5000 units SQ q8h
If contraindicated:
SCDs
Nursing
Fall precautions
Delirium precautions
Aspiration precautions PRN
Smoking cessation counseling
Ambulate TID
Incentive spirometry q1h while awake
Diet
Regular diet
Cardiac diet if indicated
NPO only if concern for intubation
Discharge
Ambulatory O2 evaluation
Pulmonary rehab referral
Ensure LABA/LAMA ± ICS prescribed
Inhaler teaching
Smoking cessation counseling
PCP follow-up within 1 week
Pulmonology follow-up if severe COPD
Meds
Home: Trelegy (ICS [fluticasone] / LABA [vilanterol] / LAMA [umeclidinium])
Inpatient: Dulera (ICS [mometasone] / LABA [formoterol]) + Spiriva (LAMA [tiotropium])
ICU: Budesonide (ICS [budesonide]) + scheduled Duoneb (SABA [albuterol] / SAMA [ipratropium], nebulized).
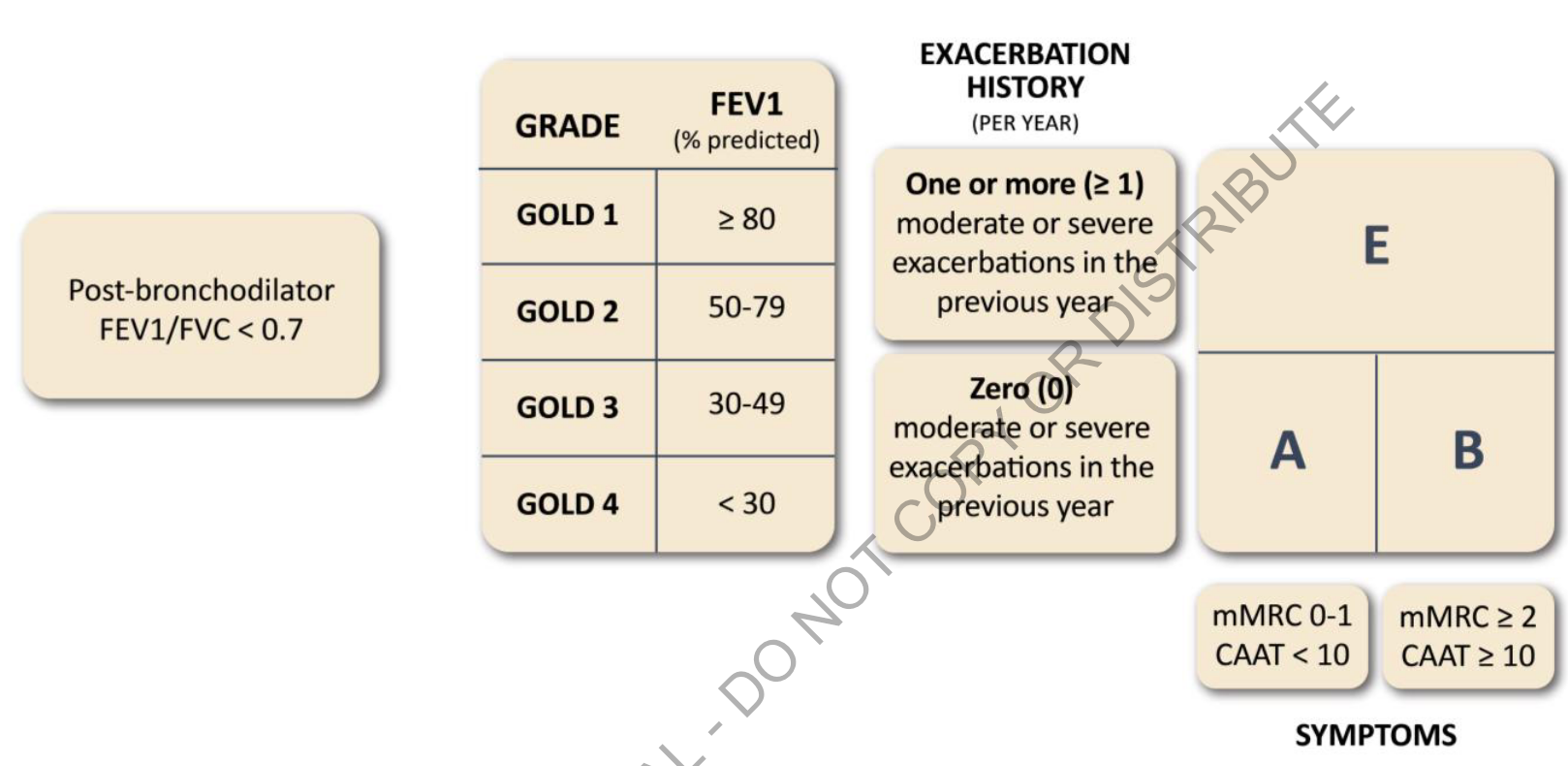
mMRC 0–1 → A
mMRC ≥2 → B
Exacerbations → E