Decompensated Cirrhosis
Cirrhosis with new ascites, variceal bleed, hepatic encephalopathy, jaundice, AKI/HRS, or infection.
Symptoms / Associated Sx
Abdominal distension/girth, ascites, early satiety, bloating, weight gain
Abdominal pain/tenderness ± fever/chills → SBP
Dyspnea → tense ascites/hepatic hydrothorax
BLE edema, jaundice/scleral icterus, pruritus
Confusion, sleep-wake reversal, asterixis → HE
Hematemesis/melena → variceal bleed
Poor PO intake, sarcopenia/muscle wasting
Denies
Hematemesis/melena — rules out active GI/variceal bleed
Fever/abdominal pain — lowers SBP likelihood but still needs paracentesis if hospitalized with ascites
Dysuria/cough — rules out UTI/PNA as precipitant
NSAID/aminoglycoside/contrast use — rules out iatrogenic AKI
Severe rebound/rigidity — if present, think secondary peritonitis/perforation
Social History (SHx)
Alcohol use/relapse, IV drug use, HBV/HCV risk, NASH/MASLD risk, known cirrhosis date/etiology, prior decompensations, prior SBP, variceal bleed, HE, med adherence, transplant/hepatology follow-up.
Main Etiology
Alcohol-related cirrhosis
MASLD/NASH
Chronic HBV/HCV
Autoimmune hepatitis, PBC, PSC
Hemochromatosis, Wilson disease, alpha-1 antitrypsin deficiency
Main Precipitants
Infection/SBP
GI bleed
Alcohol relapse
Medication noncompliance
AKI/HRS
Constipation
Electrolyte abnormalities
Portal vein thrombosis
Sedatives/opioids/benzos
Most Common DDx
Cardiac ascites/congestive hepatopathy — JVD, BNP ↑, SAAG ≥1.1 + ascitic protein >2.5
Malignant ascites — weight loss, SAAG <1.1, cytology positive
Budd-Chiari — painful hepatomegaly, ascites, Doppler hepatic vein thrombosis
Acute liver failure — INR >1.5 + HE without known cirrhosis
Alcoholic hepatitis — acute jaundice, AST >2:1
Secondary peritonitis — polymicrobial, glucose <50, LDH high, severe peritoneal signs
DATA
CBC — leukocytosis/SBP, anemia/GI bleed, thrombocytopenia/portal HTN
CMP/BMP — Cr/AKI/HRS, Na/hyponatremia, K/Mg, AST/ALT, ALP, bilirubin
PT/INR — synthetic function/coagulopathy
Albumin — synthetic function + SAAG calculation
MELD-Na + Child-Pugh score
Ammonia if AMS — supportive only, not diagnostic
Lactate if sepsis concern
Blood cultures ×2 if febrile/SBP/sepsis concern
UA/urine culture if urinary symptoms or infection concern
Diagnostic paracentesis: cell count + diff/PMN, culture in blood culture bottles, albumin, total protein
Add-ons if indicated: glucose/LDH, cytology, amylase, AFB/ADA
Serum albumin for SAAG
RUQ ultrasound + Doppler — ascites, cirrhosis morphology, portal/hepatic vein thrombosis
CXR — PNA, hepatic hydrothorax
CT abdomen/pelvis if unclear diagnosis, malignancy, secondary peritonitis, complication
AFP + HCC surveillance status
EGD status for variceal screening
Home Meds
Spironolactone/furosemide — assess dose/adherence; hold if AKI, severe hypoNa, hypotension
Lactulose/rifaximin — assess adherence
Nonselective beta blocker — hold if SBP <90, MAP low, AKI, active SBP/sepsis
SBP prophylaxis — ciprofloxacin/TMP-SMX/norfloxacin
Antivirals for HBV/HCV — usually continue
NSAIDs — stop
Opioids/benzos — avoid/hold if HE
ACEi/ARB/metformin — hold if AKI/hypotension/lactic acidosis concern
Assessment
Decompensated cirrhosis with ascites ± SBP/HE/AKI.
Need to identify precipitant: infection, GI bleed, medication noncompliance, AKI/HRS, alcohol relapse, constipation, electrolyte abnormality, PVT.
Calculate MELD-Na and Child-Pugh.
Diagnostic paracentesis required in all hospitalized patients with ascites.
Plan
F/U ordered labs, cultures, paracentesis studies, RUQ US/Doppler, CXR/CT if ordered
Diagnostic paracentesis ASAP in all hospitalized patients with ascites; do not delay for INR/thrombocytopenia
Send ascitic: cell count/diff, culture in blood culture bottles, albumin, total protein
Add glucose/LDH if secondary peritonitis concern; cytology if malignancy concern; amylase if pancreatic; AFB/ADA if TB concern
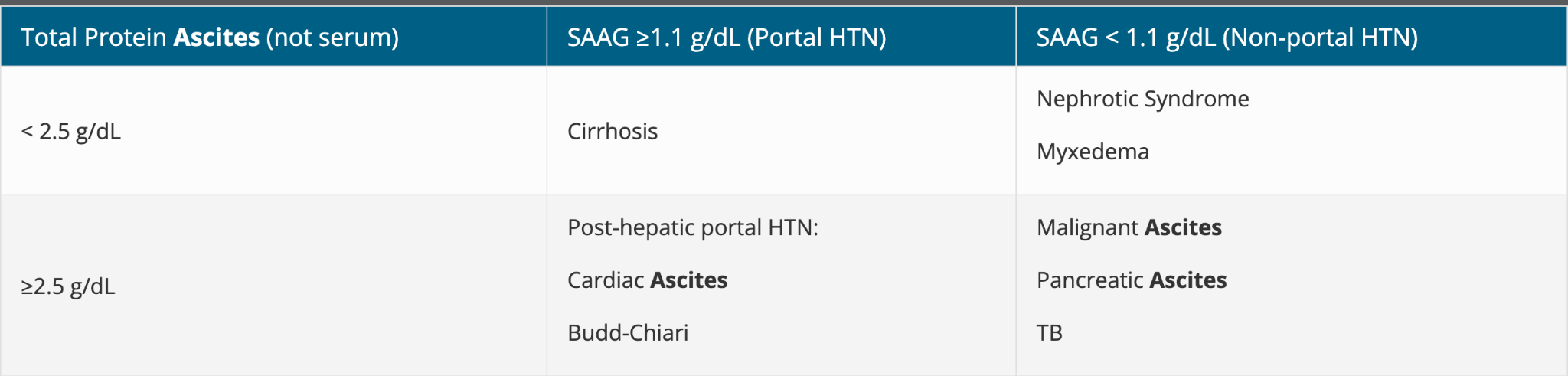
SAAG = serum albumin − ascitic albumin
SAAG ≥1.1 → portal HTN
SAAG <1.1 → malignancy/TB/pancreatic/nephrotic
SAAG ≥1.1 + protein <2.5 → cirrhosis
SAAG ≥1.1 + protein >2.5 → cardiac ascites/Budd-Chiari
Ascites
Sodium restriction <2 g/day
Fluid restriction only if severe hyponatremia, usually Na <125–130
Start/continue diuretics if renal function stable:
Spironolactone 100 mg PO daily
Furosemide 40 mg PO daily
Keep 100:40 ratio
Max spironolactone 400 mg/day + furosemide 160 mg/day
Goal weight loss:
≤0.5 kg/day if no edema
≤1 kg/day if edema present
Hold diuretics if:
Cr rises >50% or significant AKI
Na <130 or severe hypoNa
hypotension/sepsis/SBP
Daily weight, strict I/O, abdominal girth
Trend BMP/Mg daily and replete electrolytes
Large Volume Paracentesis
Perform LVP if tense ascites, dyspnea, pain, poor PO, or respiratory compromise
If >5 L removed:
Albumin 25% 6–8 g per liter removed
Example: 8 L removed → give 48–64 g albumin
Consider TIPS if refractory ascites requiring repeated LVP despite optimized diuretics
Refer hepatology/transplant if recurrent decompensation or refractory ascites
SBP
Diagnose SBP if ascitic PMN ≥250/mm³
Treat immediately; do not wait for culture
Community-acquired SBP:
Ceftriaxone 2 g IV daily × 5 days
OR Cefotaxime 2 g IV q8h × 5 days
If healthcare-associated, prior quinolone prophylaxis, septic shock, MDR/ESBL risk:
Piperacillin-tazobactam 3.375–4.5 g IV q6–8h
Consider meropenem if ESBL/MDR risk or worsening
Albumin for SBP:
1.5 g/kg IV day 1
1 g/kg IV day 3
Especially important if Cr >1, BUN >30, or bilirubin >4
Repeat paracentesis at 48 hr if severe illness, persistent fever, bacteremia, worsening status, or resistant organism concern
PMN should decrease by ≥25%; if not, broaden antibiotics and evaluate secondary peritonitis
Secondary SBP prophylaxis after any SBP episode:
Ciprofloxacin 500 mg PO daily
OR TMP-SMX DS 1 tab PO daily
Continue indefinitely until transplant or ascites resolves
Hepatic Encephalopathy
Identify/treat precipitant: SBP, GI bleed, constipation, AKI, hypokalemia, infection, sedatives, alcohol relapse
Lactulose:
20–30 g PO/NG q1–2 hr until 2–3 soft BMs
Then titrate to 2–3 BM/day
If unable PO: lactulose enema 300 mL + 700 mL water PR
Rifaximin:
550 mg PO BID if recurrent HE or inadequate response
Avoid benzos/opioids
If severe agitation: low-dose haloperidol 0.5–1 mg PO/IV cautiously
Protein restriction is outdated; goal protein 1.2–1.5 g/kg/day
Aspiration precautions, HOB elevated
ICU/intubation if grade III–IV HE, coma, or unable to protect airway
AKI / HRS Concern
Hold diuretics, NSAIDs, ACEi/ARB, nephrotoxins
Rule out infection/SBP, hypovolemia, obstruction, ATN
Albumin challenge if HRS concern
If HRS suspected:
Albumin + vasoconstrictor therapy
ICU norepinephrine if shock/ICU
Midodrine + octreotide if floor and terlipressin unavailable
Nephrology + hepatology consult
Transplant evaluation
Variceal Bleed Concern
If hematemesis/melena or acute Hgb drop:
NPO
2 large-bore IVs
Type/screen
Ceftriaxone 1 g IV daily × 7 days
Octreotide 50 mcg IV bolus then 50 mcg/hr infusion
IV PPI until EGD clarifies source
GI consult for EGD within 12 hr if active bleed
Transfuse goal Hgb ~7 unless massive bleed/ischemia
Consider TIPS if uncontrolled/recurrent bleed
General Cirrhosis Care
Avoid NSAIDs
Acetaminophen okay up to 2 g/day if no active heavy alcohol use
Avoid opioids/benzos when possible
Nutrition consult; high-protein diet 1.2–1.5 g/kg/day
Alcohol cessation counseling; addiction medicine if needed
Vaccines: HAV, HBV, pneumococcal, influenza
HCC surveillance: RUQ US ± AFP q6 months
EGD for variceal screening/surveillance if not up to date
Hepatology consult if not established
Transplant referral if MELD-Na ≥15, recurrent decompensation, SBP, refractory ascites, HRS, or variceal bleed
PT/OT eval and treat
Trend daily CBC, CMP, INR, Cr, electrolytes, fever curve
Follow up pending cultures, paracentesis results, imaging
Discharge Recommendations
Sodium restriction <2 g/day
Daily weights; return if rapid weight gain, worsening distension, fever, abdominal pain, confusion, melena/hematemesis, decreased urine output
Continue/titrate diuretics if renal function stable
Lactulose titrated to 2–3 soft BMs/day ± rifaximin 550 mg BID
Lifelong SBP prophylaxis if prior SBP
Avoid NSAIDs, alcohol, benzos/opioids unless absolutely necessary
Hepatology follow-up within 1–2 weeks
Ensure HCC screening q6 months and EGD surveillance
Recheck CMP/BMP/INR within 1 week if diuretics adjusted or recent AKI/SBP
Red Flags
PMN ≥250 → SBP → antibiotics + albumin immediately
Rising Cr despite albumin/holding diuretics → HRS concern
Severe abdominal pain/rebound/rigidity → secondary peritonitis → CT + surgery
Hematemesis/melena → variceal bleed pathway
Grade III–IV HE/coma → ICU/airway
MELD-Na >20–21 → high mortality; urgent hepatology/transplant discussion
Triple decompensation: GI bleed + HE + AKI → ICU/high mortality
Senior IM Resident Pearls
VIBES = decompensations:
V = Variceal bleed
I = Infection/SBP
B = Brain/HE
E = Edema/ascites
S = Synthetic dysfunction
Diagnostic paracentesis is mandatory for hospitalized cirrhotics with ascites.
PMN ≥250 = SBP; culture can be negative.
Culture ascitic fluid in blood culture bottles at bedside.
SAAG ≥1.1 = portal HTN.
SAAG ≥1.1 + protein <2.5 = cirrhosis.
SAAG ≥1.1 + protein >2.5 = cardiac/Budd-Chiari.
Albumin after LVP >5 L prevents post-paracentesis circulatory dysfunction.
Albumin in SBP prevents HRS and improves survival.
Do not restrict protein in HE; it worsens sarcopenia.
Ammonia does not track HE severity well; treat the patient, not the number.
Hold BB only when hypotension, AKI, active SBP/sepsis, or shock—not automatically in every decompensated patient.
Avoid NSAIDs always in cirrhosis; use acetaminophen ≤2 g/day.
Every SBP episode should trigger transplant/hepatology discussion.
Scores
MELD-Na
Uses bilirubin, INR, creatinine, sodium
Drives transplant priority
MELD-Na ≥15 → transplant referral
MELD-Na >20–21 → high inpatient mortality risk
MELD-Na >30 → very high short-term mortality
Child-Pugh
Uses bilirubin, albumin, INR, ascites, encephalopathy
Class A = 5–6
Class B = 7–9
Class C = 10–15
Predicts prognosis and surgical risk
West Haven HE Grade
Grade 0: none/minimal
Grade 1: sleep changes, mild confusion
Grade 2: lethargy, disorientation, asterixis
Grade 3: somnolent but arousable
Grade 4: coma
ORDERS
Labs
Admission Labs
CBC with diff
CMP
BMP
PT/INR
PTT
Albumin
Lactate
Magnesium
Phosphorus
Blood cultures ×2
Type & Screen (if concern for bleed)
Ammonia (if AMS/HE)
MELD-Na calculation
Child-Pugh calculation
Additional Labs
AFP
HBV/HCV panel if etiology unclear
Ethanol level
Urinalysis
Urine culture
Ascitic fluid studies:
Cell count + differential
Culture (in blood culture bottles)
Albumin
Total protein
Glucose
LDH
Cytology
Amylase
AFB/ADA (if indicated)
Trending Labs
CBC daily
CMP daily
BMP daily
PT/INR daily
Cr daily
Mg/Phos daily
Daily MELD-Na
Daily weights
Imaging
Initial Imaging
RUQ Ultrasound + Doppler
Ascites
Portal vein thrombosis
Hepatic vein thrombosis
Cirrhotic morphology
CXR
Pneumonia
Hepatic hydrothorax
Additional Imaging
CT Abdomen/Pelvis
If:
Secondary peritonitis
Malignancy
Unclear diagnosis
Severe abdominal pain
Procedures
Mandatory
Diagnostic Paracentesis
(All hospitalized cirrhotics with ascites)
Send:
Cell count
Differential
Culture
Albumin
Total protein
Therapeutic
Large Volume Paracentesis (LVP)
Indications:
Tense ascites
Dyspnea
Poor PO intake
Abdominal pain
Respiratory compromise
If >5 L Removed
Albumin
Albumin 25%
6–8 g per L removed
Example:
8 L removed
Give 48–64 g albumin
Medications
Ascites Management
Sodium Restriction
<2 g/day
Fluid Restriction
Only if:
Na <125–130
Diuretics
Standard Starting Ratio
Spironolactone 100 mg PO daily
Furosemide 40 mg PO daily
Maximum
Spironolactone 400 mg/day
Furosemide 160 mg/day
Hold Diuretics If
AKI
Cr rise >50%
Na <130
Hypotension
SBP
Sepsis
SBP Treatment
PMN ≥250 = SBP
Treat immediately.
First-Line
Ceftriaxone
2 g IV daily x5 days
OR
Cefotaxime
2 g IV q8h x5 days
Healthcare Associated / MDR Risk
Piperacillin-Tazobactam
4.5 g IV q6–8h
ESBL Risk
Meropenem
1 g IV q8h
Albumin for SBP
Day 1
1.5 g/kg IV
Day 3
1 g/kg IV
Especially if:
Cr >1
BUN >30
Bilirubin >4
SBP Prophylaxis
Ciprofloxacin
500 mg PO daily
OR
TMP-SMX DS
1 tab PO daily
Continue indefinitely.
Hepatic Encephalopathy
Lactulose
Acute
20–30 g PO/NG q1–2 hr until BM
Maintenance
Titrate to 2–3 soft BM/day
If Cannot Take PO
Lactulose enema
300 mL lactulose + 700 mL water PR
Rifaximin
550 mg PO BID
Agitation
Haloperidol 0.5–1 mg PO/IV PRN
Avoid
Benzos
Opioids
AKI / HRS
Hold
Diuretics
NSAIDs
ACEi
ARBs
Nephrotoxins
Albumin Challenge
If HRS suspected
Vasoconstrictors
ICU
Norepinephrine infusion
Floor
Midodrine + Octreotide
Consult
Nephrology
Hepatology
If Variceal Bleed Suspected
NPO
Two large-bore IVs
Type & Screen
Octreotide
50 mcg IV bolus
Then 50 mcg/hr infusion
Ceftriaxone
1 g IV daily x7 days
Pantoprazole
40 mg IV BID until EGD
EGD
Within 12 hr
Transfusion Goal
Hgb ~7
Hold Medications
Hold
NSAIDs
ACEi
ARBs
Aminoglycosides
Metformin (AKI/lactic acidosis concern)
Opioids
Benzodiazepines
Hold NSBB If
SBP <90
MAP low
AKI
Active SBP
Sepsis
Shock
Consults
Hepatology
(All decompensated cirrhosis)
Gastroenterology
Varices
GI bleed
EGD needs
Interventional Radiology
TIPS
Refractory ascites
Nephrology
AKI
HRS
Transplant Team
If:
MELD-Na ≥15
Recurrent decompensation
SBP
HRS
Variceal bleed
Nutrition
Sarcopenia
Malnutrition
Addiction Medicine
Alcohol use disorder
PT/OT
Deconditioning
Nursing Orders
Monitoring
Strict I&O
Daily weights
Daily abdominal girth
Fall precautions
Aspiration precautions (HE)
Diet
Sodium restriction <2 g/day
Protein 1.2–1.5 g/kg/day
No protein restriction
Notify Physician
Fever
AMS
GI bleeding
Oliguria
Worsening abdominal pain
Rapid abdominal distension
Decompensation Hx: (VIBES)
-- Volume/Ascites: prior LVP, frequency, salt restriction on lasix/spironolactone
-- Infection/SBP: prior infections, h/o low protein ascites, on ppx
-- Bleeding/EV: last EGD, prior bleeds, banding, on nadolol/PPI
-- Encephalopathy/HE: prior decompensation, on lactulose/rifaximin, BM/day
-- Screening/HCC: last screen, AFP; if nodule >1cm get multiphase CT or MRI