Anemia
MICROCYTIC (MCV <80) → TICS
-- SX:Fatigue, generalized weakness, lightheadedness, SOB/DOE, palpitations, tachycardia, angina, melena/hematochezia/hematemesis, pica, hair loss, and restless legs.
-- Hx: IDA,CKD,CKD/ESRD, Autoimmune, malignancy, GI bleed
-- PE:
-- W/U: CBC w/ diff (wbc/Hgb/platelets), Iron Deficiency Panel (ferritin,TIBC,iron), CMP(Bili), Type & screen, coags, UA, Hb electrophoresis (if thalassemia), Lead level (if sideroblastic concern)
-- MEDS:
-- DDX: TICS (Thalassemia,Iron deficiency,Chronic disease,Sideroblastic
Plan
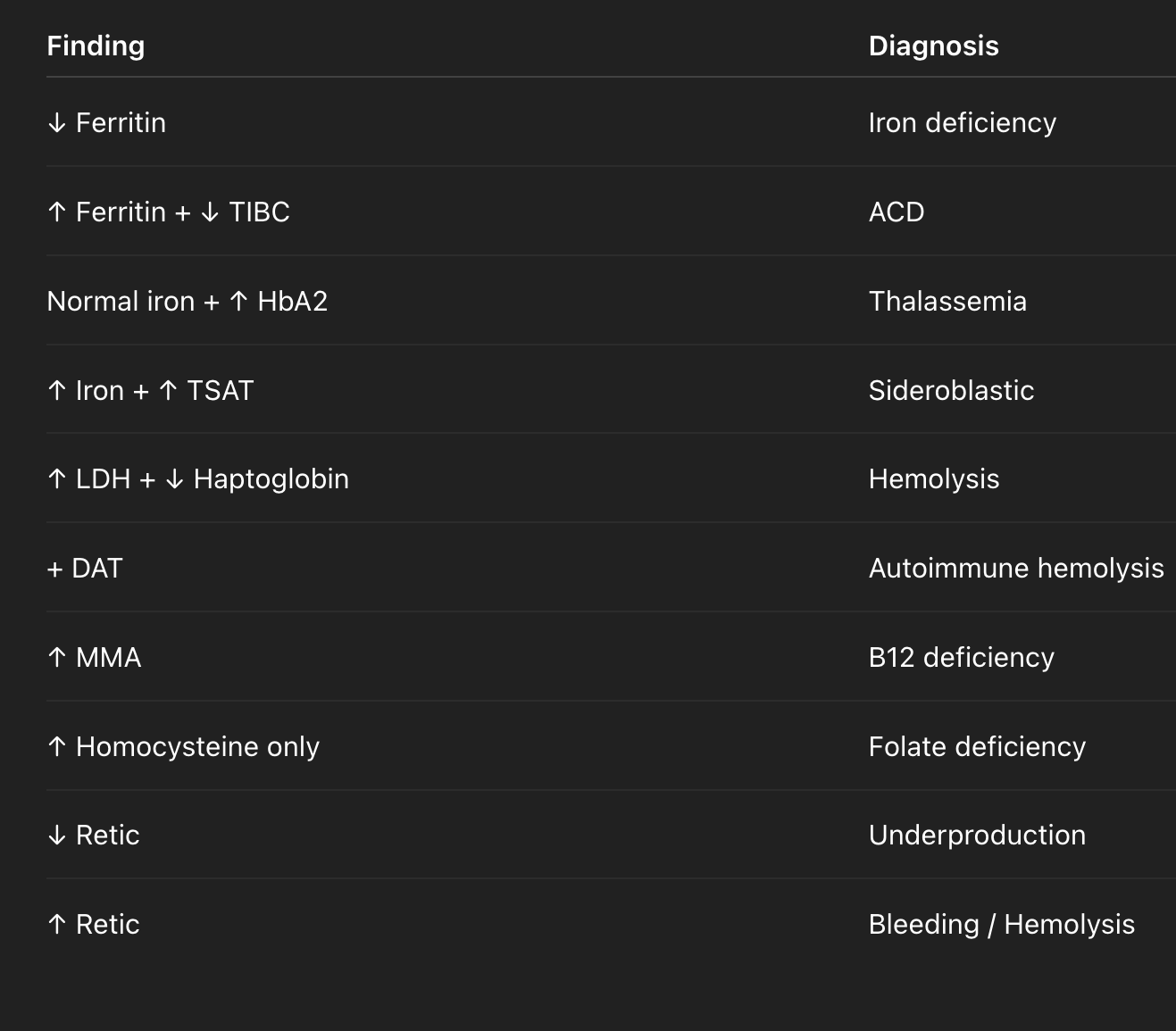
-- IDA - (↓ ferritin, ↓ serum iron, ↑ TIBC, ↓ transferrin saturation (<15–20%) Ferric gluconate: 250 mg IV daily or twice daily (total ~1000 mg over 4-8 days). , Ferrous sulfate 325 mg daily on DC
-- Thalassemia (Normal or ↑ ferritin, normal iron, normal TIBC, abnormal Hb electrophoresis (↑ HbA2 ± HbF)-> Tx hematology referral , Usually no treatment, transfuse PRN
-- Anemia of chronic disease (Normal/↑ ferritin, ↓ serum iron, ↓ TIBC, ↓ transferrin saturation) (CKD, infection, cancer, autoimmune) -> tx CKD (EPO),Tx underlying cause
-- Sideroblastic anemia (alcohol/lead poisoning) (↑ ferritin, ↑ serum iron, ↓/normal TIBC, ↑ transferrin saturation >45–50% ± ring sideroblasts on marrow) tx: Pyridoxine (Vitamin B6) 200 mg daily (specialy INH-induced), Stop offending agents (alcohol, meds), transfuse PRN, correct iron overload iron chelation with deferasirox 10-20 mg/kg PO daily or deferoxamine 20-40 mg/kg SC/IV when ferritin >1000 ng/mL
-- transfuse Hgb <7 or (<8 if CAD/symptomatic/Perioperative)
-- transfuse plt if <10k or <20k→ if fever/sepsis or <50k→ if active bleeding
Anemia
NORMOCYTIC (MCV 80–100)
-- SX: Fatigue, generalized weakness, lightheadedness, SOB/DOE, palpitations, tachycardia, angina, melena/hematochezia/hematemesis, pica, hair loss, and restless legs.
-- Hx: CKD/ESRD, Autoimmune, malignancy, GI bleed,
-- PE:
-- W/U: CBC w/ diff (wbc/Hgb/platelets),retic count, Iron Deficiency Panel (ferritin,TIBC,Iron), CMP(Bili), Type & screen, Peripheral smear, [LDH, haptoglobin], DAT (Coombs)?, coags, UA,
-- MEDS:
-- DDX: LOW RETIC/UNDERPRODUCTION -> Anemia of Chronic Disease ((CKD,infection, cancer, autoimmune),Bone marrow failure (aplastic, malignancy), HIGH RETIC = LOSS OR DESTRUCTION -> Bleeding vs Hemolysis
Plan
-- Anemia of Chronic Disease (CKD, infection, cancer, autoimmune) low retic, ↑ ferritin->CKD (EPO),Tx underlying cause
-- Aplastic anemia->Pancytopenia (pancytopenia)->hematology for immunosuppression or transplant (Aplastic) or chemo for (Malignancy)
-- Bleeding-Related Anemia-> (history + ↓ Hb) -> stop bleeding / transfuse ((GI BLEED))
-- Hemolytic Anemia (↑ LDH,↑ indirect bilirubin,↓ haptoglobin) -> consult hematology for Tx Autoimmune/Steroids, TTP/HUS/Plasma exchange (urgent), G6PD/avoid triggers ((Hemolytic anemia/Thrombocytopenia))
-- transfuse Hgb <7 or (<8 if CAD/symptomatic/Perioperative)
-- transfuse plt if <10k or <20k→ if fever/sepsis or <50k→ if active bleeding
-- ESRD - EPO
Anemia
MACROCYTIC (MCV >100)
-- SX:Fatigue, generalized weakness, lightheadedness, SOB/DOE, palpitations, tachycardia, angina, melena/hematochezia/hematemesis, pica, hair loss, and restless legs.
-- Hx:B12/Folate deficiency,Alcohol history,liverdisease,Hypothyroidism
-- PE:
-- W/U: CBC,CMP(LFT), TSH, B12,Folate, MMA, [Retic count, LDH, haptoglobin, Bili]
-- MEDS:_Methotrexate, hydroxyurea, zidovudine (AZT), chemo agents, and anticonvulsants (phenytoin, valproate)
-- DDX: MEGALOBLASTIC (hypersegmented neutrophils + macro-ovalocytes)->(B12 deficiency,Folate deficiency), NON-MEGALOBLASTIC(Alcohol, Liver disease, Hypothyroidism, Medications) ALSO hemolysis (indirectly-> ↑ reticulocytes (larger than RBCs → mild macrocytosis)
Plan
-- B12 ↓ → MMA ↑ + homocysteine ↑-> 1000 mcg IM daily × 3–7 days, then weekly until improvement
-- Folate ↓ → homocysteine ↑, MMA normal -> Folic acid 1 mg PO daily If NPO → 1 mg IV
-- AUD-> Thiamine IV (200 mg IV for 3 days then 100 mg daily on DC) + Prenatal vitamin or MVI daily
-- Hypothyroidism-> Tx underlying cause
-- Hemolytic Anemia (↑ LDH,↑ indirect bilirubin,↓ haptoglobin) -> consult hematology for Tx Autoimmune/Steroids, TTP/HUS/Plasma exchange (urgent), G6PD/avoid triggers ((Hemolytic anemia/Thrombocytopenia))
-- transfuse Hgb <7 or (<8 if CAD/symptomatic/Perioperative)
-- transfuse plt if <10k or <20k→ if fever/sepsis or <50k→ if active bleeding