Acute Cholecystitis
Acute gallbladder inflammation from cystic duct obstruction — calculous (90%) or acalculous (critically ill)
Symptoms / Associated Sx
RUQ or epigastric pain — constant, worsening over hours (unlike biliary colic which waxes/wanes)
Fever, chills, nausea, vomiting, anorexia
Murphy's sign (inspiratory arrest with deep RUQ palpation)
RUQ tenderness with guarding
Denies
Jaundice (rules out concurrent CBD stone/cholangitis if absent)
Fever + jaundice + RUQ pain together (raises cholangitis, not isolated cholecystitis)
Hemodynamic instability (rules out gangrenous/emphysematous if absent — do not be falsely reassured)
Social History (SHx)
"5 Fs" risk factors (female, fat, forty, fertile, fair), prior biliary colic, prolonged fasting/TPN (acalculous), ICU admission, sickle cell disease, rapid weight loss.
Main Etiology
Calculous (90%): cystic duct obstruction by gallstone → bile stasis → inflammation → secondary infection
Acalculous (10%): critically ill (ICU, TPN, burns, major surgery) — bile stasis without stones; higher mortality
Gangrenous: necrosis — diabetics, elderly, delayed presentation
Emphysematous: gas-forming organisms (Clostridium, E. coli) — diabetics; surgical emergency
Most Common DDx
Acute cholangitis (RUQ pain + fever + jaundice = Charcot's triad; CBD dilation with stone; CBD dilated vs. normal in isolated cholecystitis)
Acute pancreatitis (epigastric pain radiating to back; lipase >3× ULN; may coexist — check both; no Murphy's sign)
Perforated peptic ulcer (sudden-onset severe epigastric pain; free air on imaging; rigid abdomen; no Murphy's sign)
Appendicitis (RLQ pain; migration from periumbilical; rebound at McBurney's; CT confirms; no biliary findings)
Hepatic abscess (fever + RUQ pain; CT shows hypodense collection in liver parenchyma; gallbladder normal)
Right lower lobe pneumonia (fever + RUQ/right-sided pain from diaphragmatic irritation; CXR consolidation; no gallbladder findings)
Acalculous cholecystitis (same presentation but no stones on US; critically ill patients; HIDA confirms; higher mortality)
DATA
CBC (WBC >10k); CMP (LFTs, bilirubin — if elevated, suspect CBD stone); lipase (concurrent pancreatitis); PT/INR
Blood cultures (if febrile + systemic signs)
RUQ ultrasound (first-line: gallstones, wall thickening >4 mm, pericholecystic fluid, sonographic Murphy's)
HIDA scan (gold standard — non-visualization of GB = cystic duct obstruction; use if US equivocal)
CT (complications — gangrenous, emphysematous, perforation)
Home Meds
Anticoagulants (hold; reverse for emergent surgery); antiplatelets (hold 5–7 days)
Diabetes medications (hold during NPO)
Plan
NPO; IV fluid resuscitation; analgesia (ketorolac 15–30 mg IV q6h ± hydromorphone 0.2–0.4 mg IV q4h PRN)
Antibiotics:
Mild (TG I): Cefazolin 1–2 g IV q8h or ampicillin-sulbactam 3 g IV q6h
Moderate (TG II): Piperacillin-tazobactam 3.375 g IV q6h
Severe/complicated/healthcare-associated: Meropenem 1 g IV q8h ± Vancomycin
Cholecystectomy:
Laparoscopic — preferred; early surgery (<72h) reduces complications and LOS
High surgical risk: percutaneous cholecystostomy → interval cholecystectomy at 6–8 weeks
Gangrenous or emphysematous → emergent surgery
Surgery consult immediately; daily CBC, CMP, LFTs; trend fever curve
PT/OT pre- and post-operatively
Discharge: Low-fat diet × 4–6 weeks; return precautions: fever, worsening pain, jaundice; surgery follow-up 2–4 weeks; if cholecystostomy tube: interval cholecystectomy scheduling 6–8 weeks
Red Flags
Emphysematous cholecystitis (gas in GB wall on CT) → emergent surgery; high mortality in diabetics
Gangrenous cholecystitis → emergent surgery; clues: severe pain, WBC >20k, diabetes, elderly
Gallbladder perforation → emergent surgery + IR drainage
Charcot's triad = cholangitis complicating cholecystitis → ERCP + antibiotics urgently
Acalculous cholecystitis in ICU → high index of suspicion; HIDA or CT; percutaneous cholecystostomy if too ill
Senior IM Resident Pearls
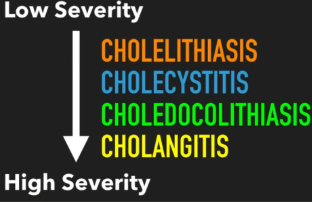
Tokyo Guidelines 2018 grade severity: Grade I = mild; Grade II = moderate (local complications); Grade III = severe (organ failure) — drives surgical urgency
Early laparoscopic cholecystectomy (<72h) is superior to delayed — reduces LOS by 3–4 days, reduces readmissions (ACDC trial)
HIDA scan most sensitive/specific when US equivocal — non-filling of GB at 4h = cystic duct obstruction
Acalculous cholecystitis — higher morbidity/mortality; occurs in burns, post-op, TPN, sepsis; lower threshold for diagnosis in ICU patients with unexplained fever
Common mistake: Delaying cholecystectomy for "cooling off" — early surgery is now standard of care
Common mistake: Attributing all LFT elevation to cholecystitis — any jaundice or CBD dilation → MRCP/ERCP to rule out Mirizzi syndrome or choledocholithiasis
ORDERS
Labs
Admission Labs
CBC with diff
CMP
BMP
LFTs (AST, ALT, ALP, GGT, total/direct bilirubin)
PT/INR
PTT
Lipase
Magnesium
Phosphorus
Additional Labs
Blood cultures ×2 (if febrile/systemic signs)
Lactate (sepsis concern)
Type & Screen (operative planning)
HbA1c if diabetes history
Trending Labs
CBC daily
CMP daily
LFTs daily
BMP daily
Fever curve
Blood culture results
Imaging
First-Line
RUQ Ultrasound
Evaluate:
Gallstones
Gallbladder wall thickening (>4 mm)
Pericholecystic fluid
Sonographic Murphy sign
CBD dilation
If Ultrasound Equivocal
HIDA Scan
Gold standard:
Nonvisualization of gallbladder
Cystic duct obstruction
If Complications Suspected
CT Abdomen/Pelvis with Contrast
Evaluate:
Gangrenous cholecystitis
Emphysematous cholecystitis
Perforation
Abscess
If CBD Stone Suspected
MRCP
OR
ERCP
If:
Jaundice
Elevated bilirubin
CBD dilation
Procedures
Surgery (Definitive)
Laparoscopic Cholecystectomy
Preferred:
Within 72 hr of symptom onset
Same hospitalization
High Surgical Risk
Percutaneous Cholecystostomy Tube
IR placement
Interval cholecystectomy in 6–8 weeks
Emergent Surgery
Indications:
Gangrenous cholecystitis
Emphysematous cholecystitis
Perforation
Sepsis with source not controlled
Medications
Supportive Care
NPO
IV Fluids
LR Preferred
100–150 mL/hr
Additional boluses PRN
Pain Control
First-Line
Ketorolac 15–30 mg IV q6h PRN
Severe Pain
Hydromorphone 0.2–0.4 mg IV q4h PRN
Alternative
Oxycodone 5–10 mg PO q4–6h PRN
Antiemetics
Ondansetron
4 mg IV q6h PRN
Antibiotics
Mild (Tokyo Grade I)
Cefazolin
1–2 g IV q8h
OR
Ampicillin-Sulbactam
3 g IV q6h
Moderate (Tokyo Grade II)
Piperacillin-Tazobactam
4.5 g IV q6h
Severe / Complicated / HCAI
Meropenem
1 g IV q8h
Add Vancomycin If
MRSA risk
Healthcare-associated infection
Vancomycin
15–20 mg/kg IV q8–12h
Duration
Uncomplicated
Usually stop within 24 hr after cholecystectomy
Severe/Complicated
4–7 days after source control
Hold Medications
Before Surgery
Warfarin
DOACs
Heparin
Clopidogrel
Ticagrelor
Hold While NPO
Oral diabetes medications
Consults
General Surgery (Immediate)
All confirmed cholecystitis
Gastroenterology
If:
Suspected choledocholithiasis
Elevated bilirubin
CBD dilation
Need ERCP
Interventional Radiology
Cholecystostomy tube
Poor operative candidate
ICU
If:
Organ failure
Septic shock
Gangrenous disease
PT/OT
Pre-op/post-op mobility
Deconditioning
Nursing Orders
Monitoring
Vital signs q4 hr
Strict I&O
Daily weights
Diet
NPO until surgical plan established
Notify Physician Immediately
Fever
Hypotension
Jaundice
Worsening RUQ pain
AMS